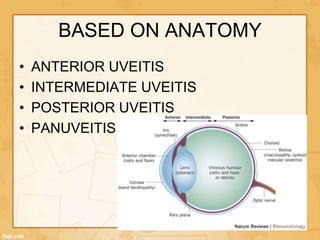
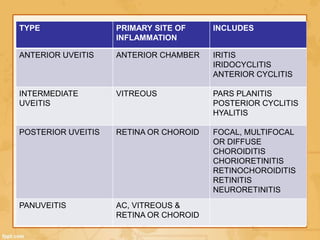
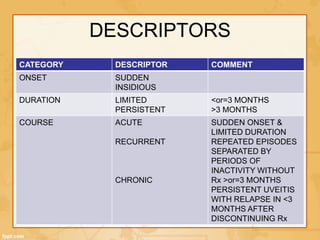
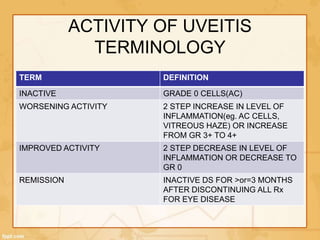
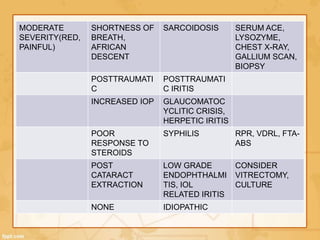
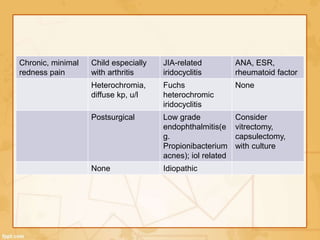
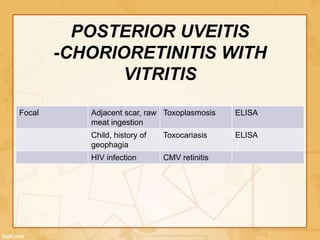
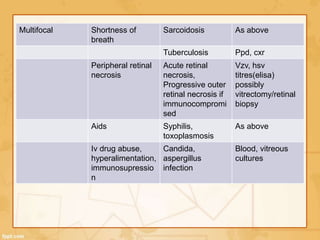
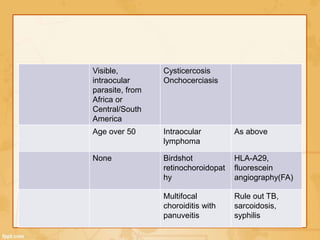
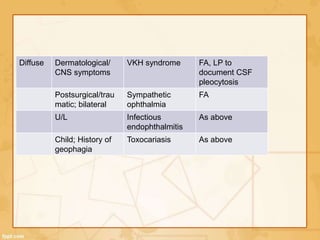
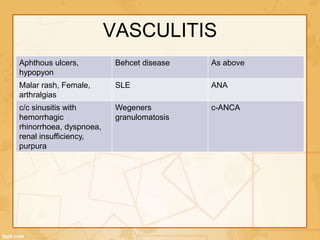
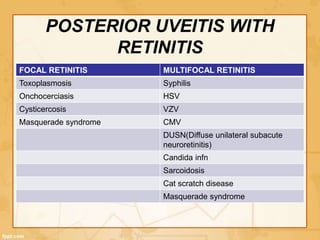
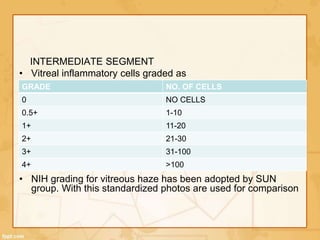
Uveitis is classified based on the primary site of inflammation in the eye: anterior, intermediate, posterior, or panuveitis. It is also described based on clinical features like onset, duration, and course. A thorough evaluation is needed to categorize uveitis and identify any underlying etiology, as it can be associated with systemic diseases. A standardized system of nomenclature exists to describe uveitis uniformly based on anatomy, activity, and other characteristics. Symptoms depend on the location and severity of inflammation, and may include pain, photophobia, blurred vision, or floaters.