Downloaded 123 times
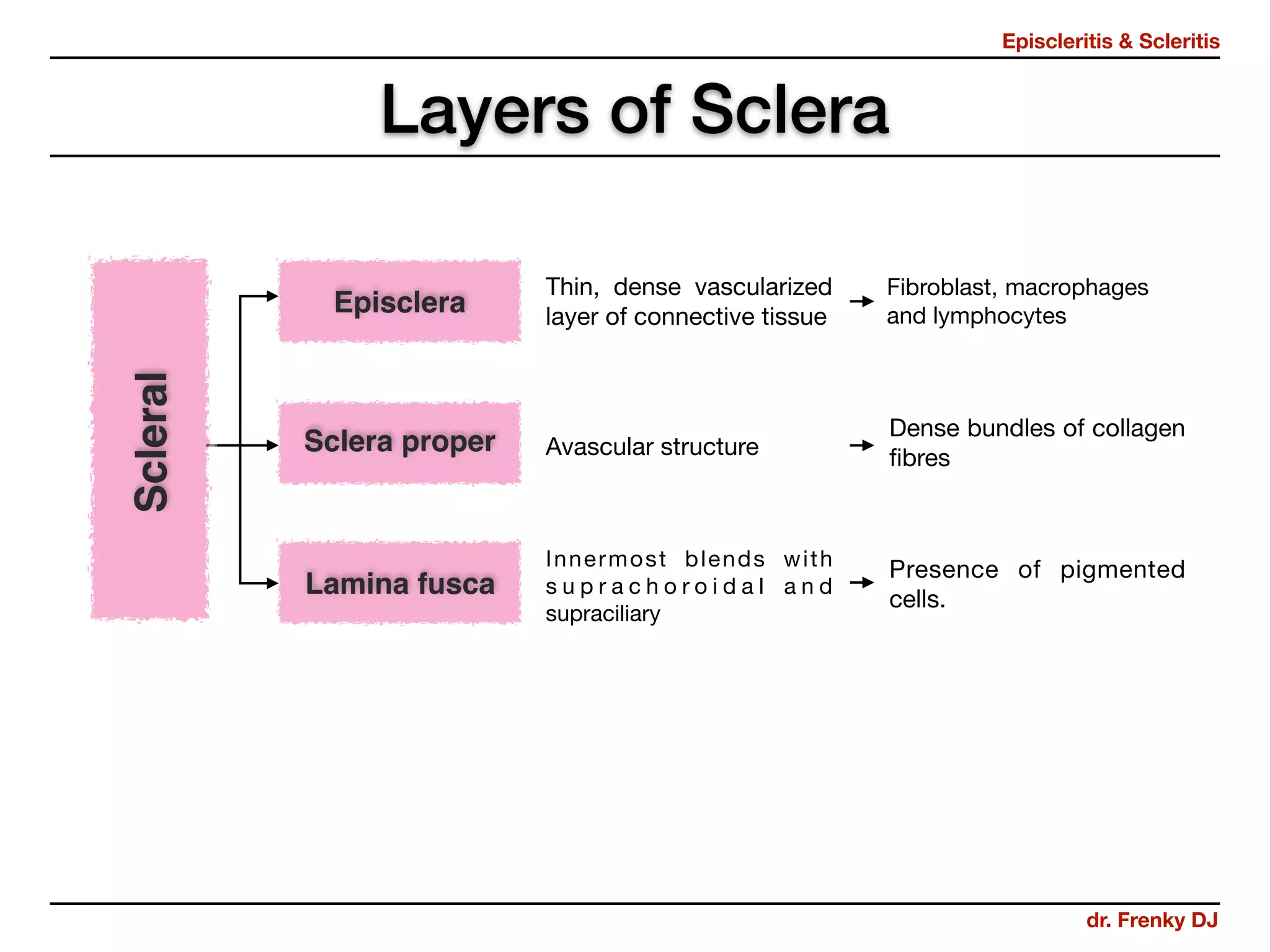
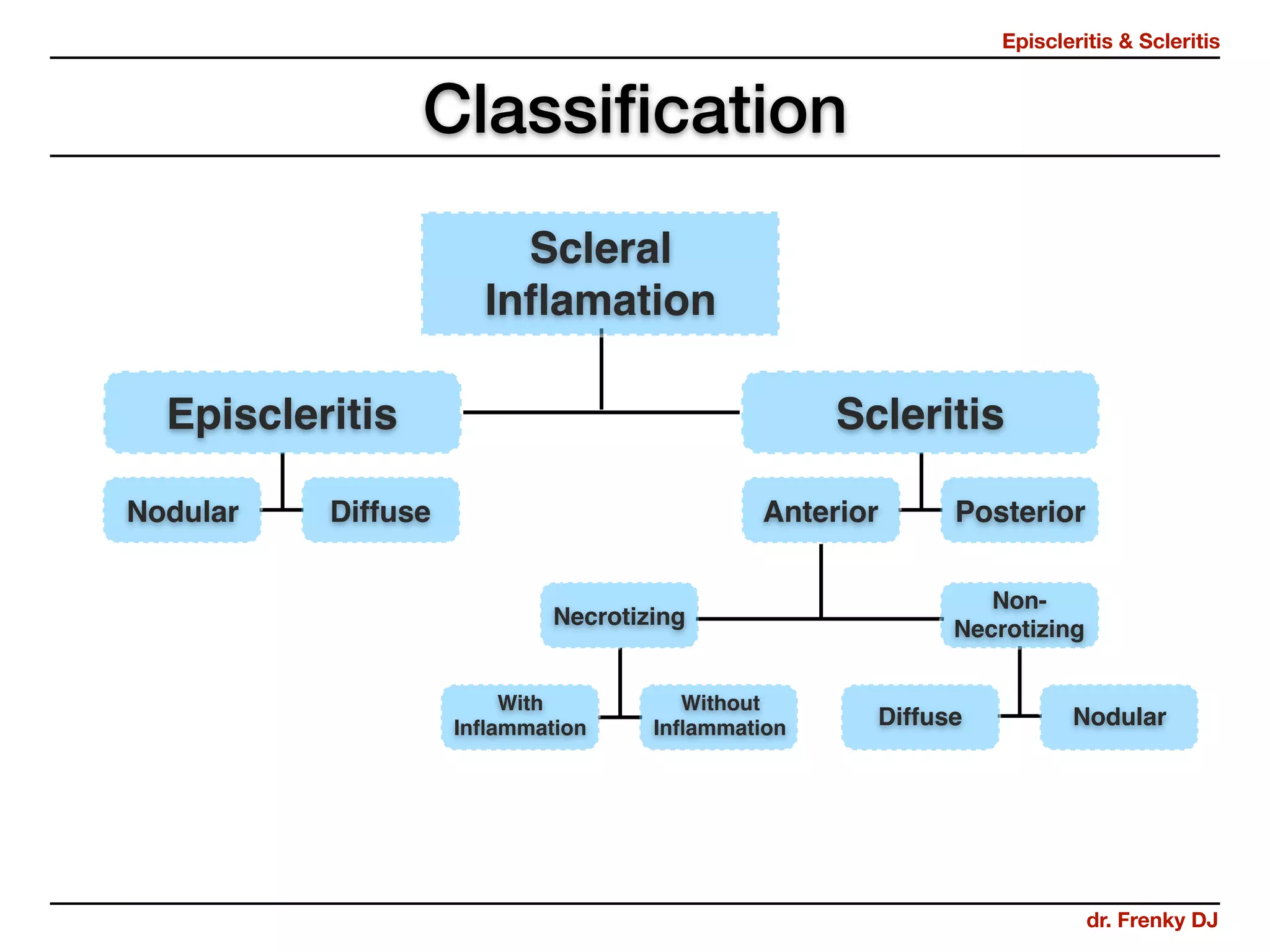
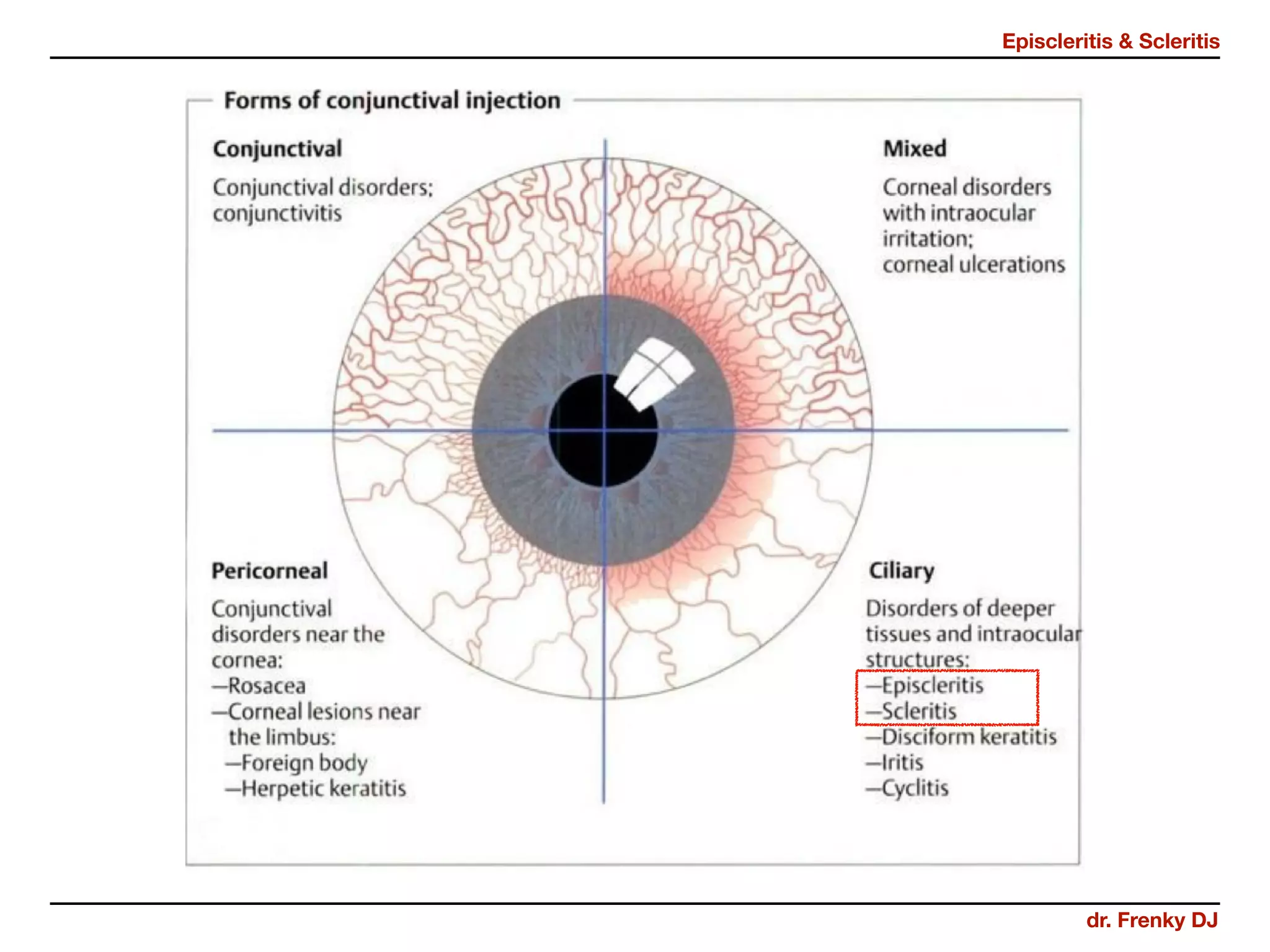




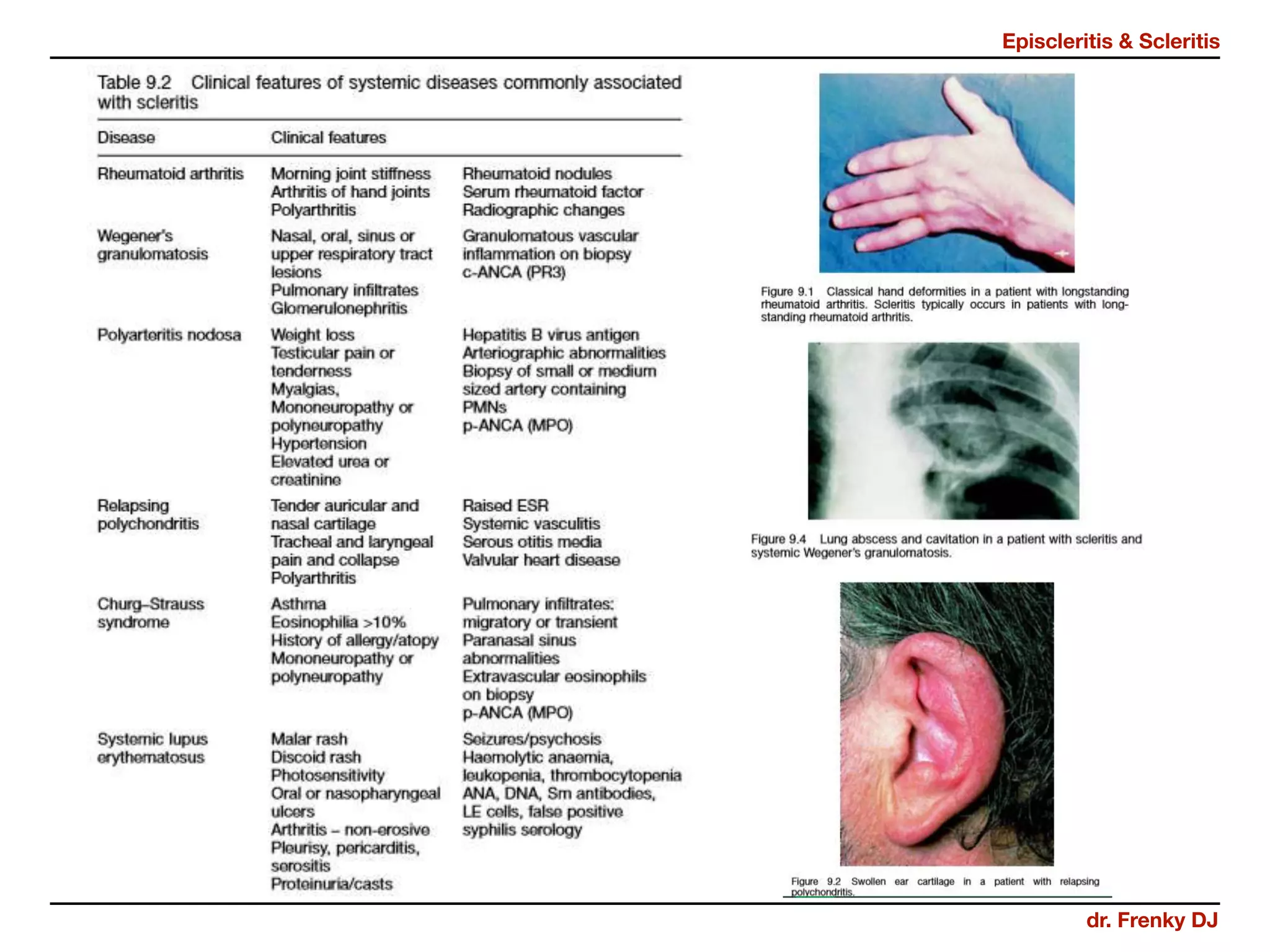




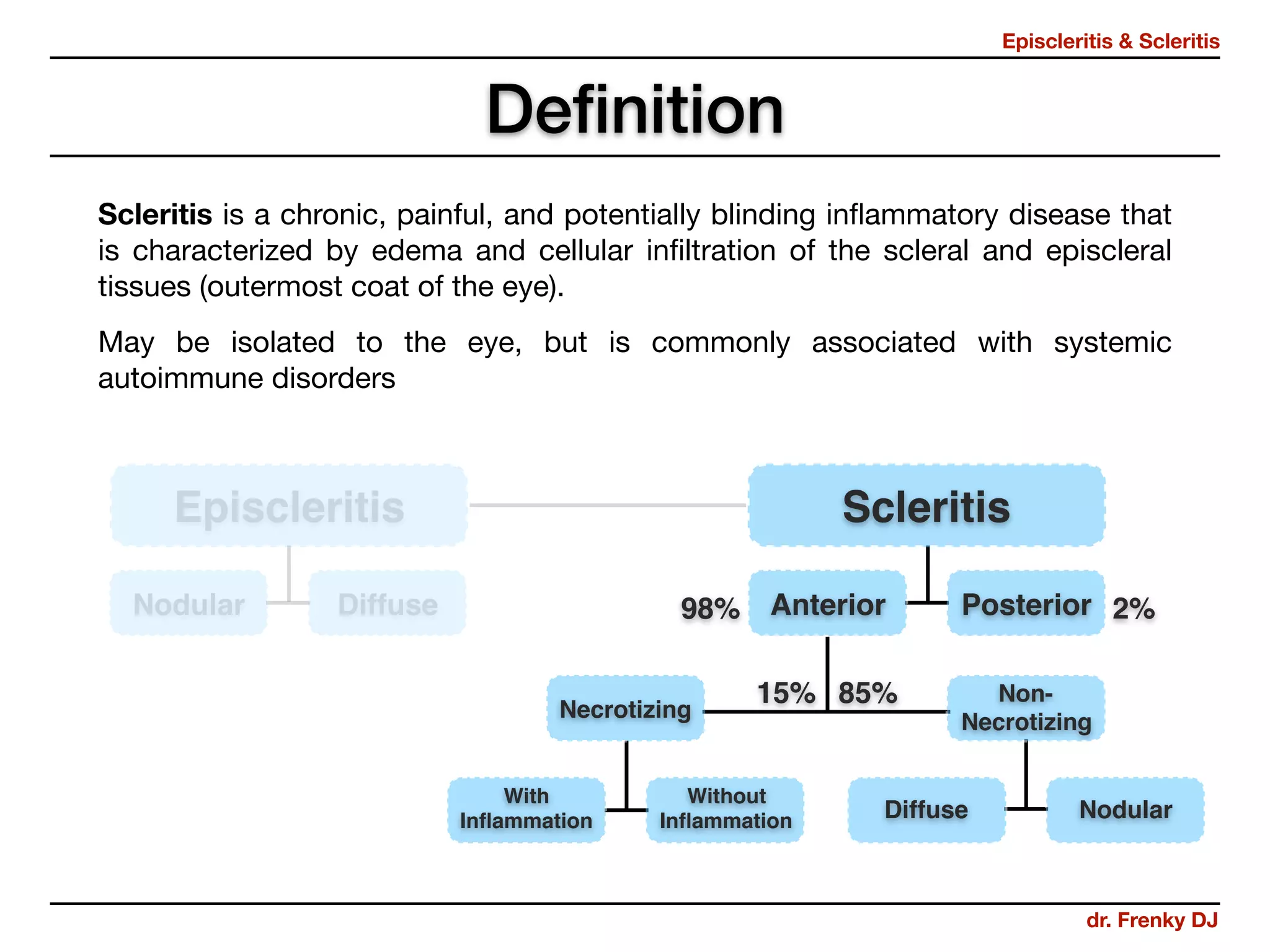
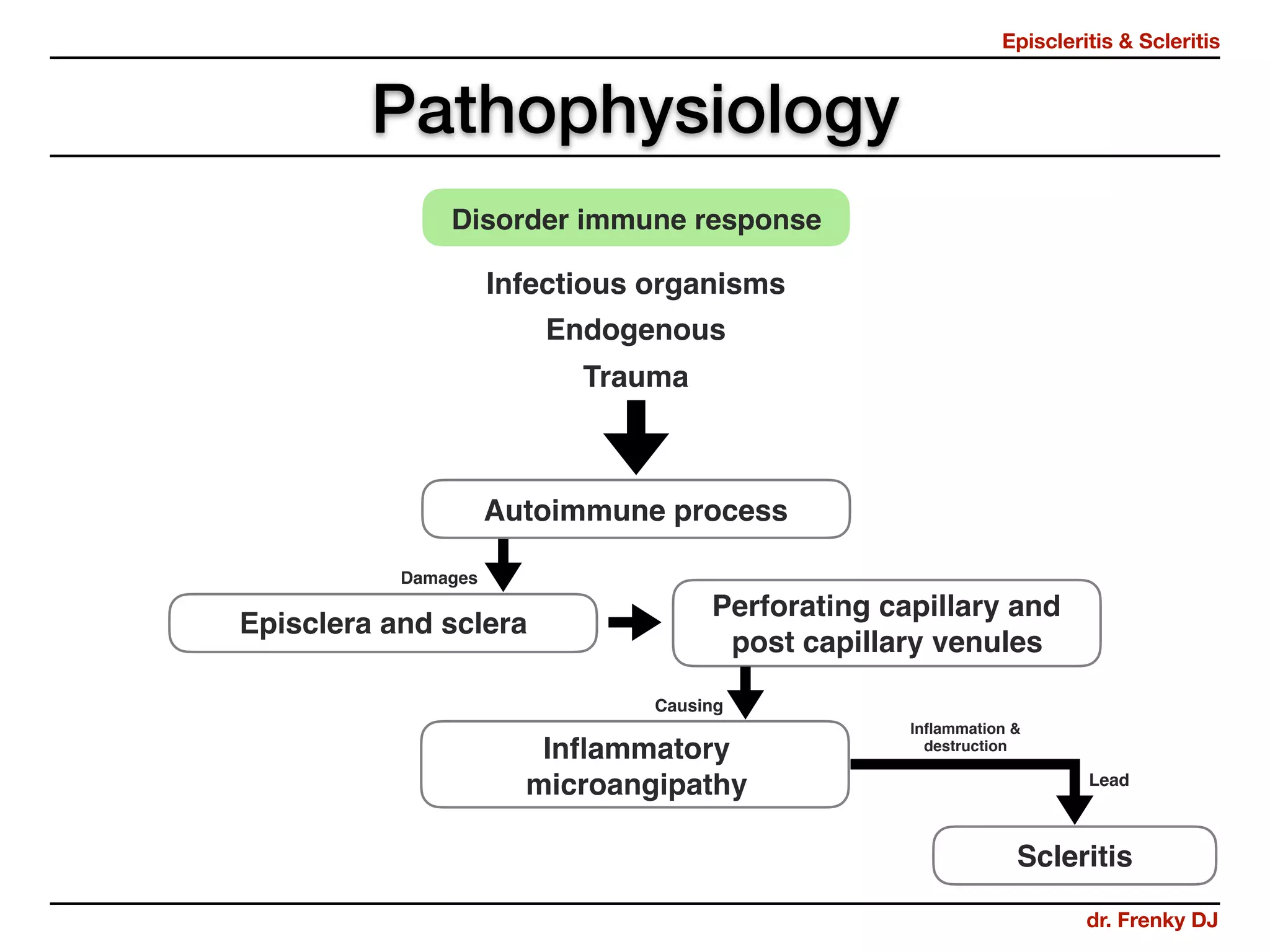






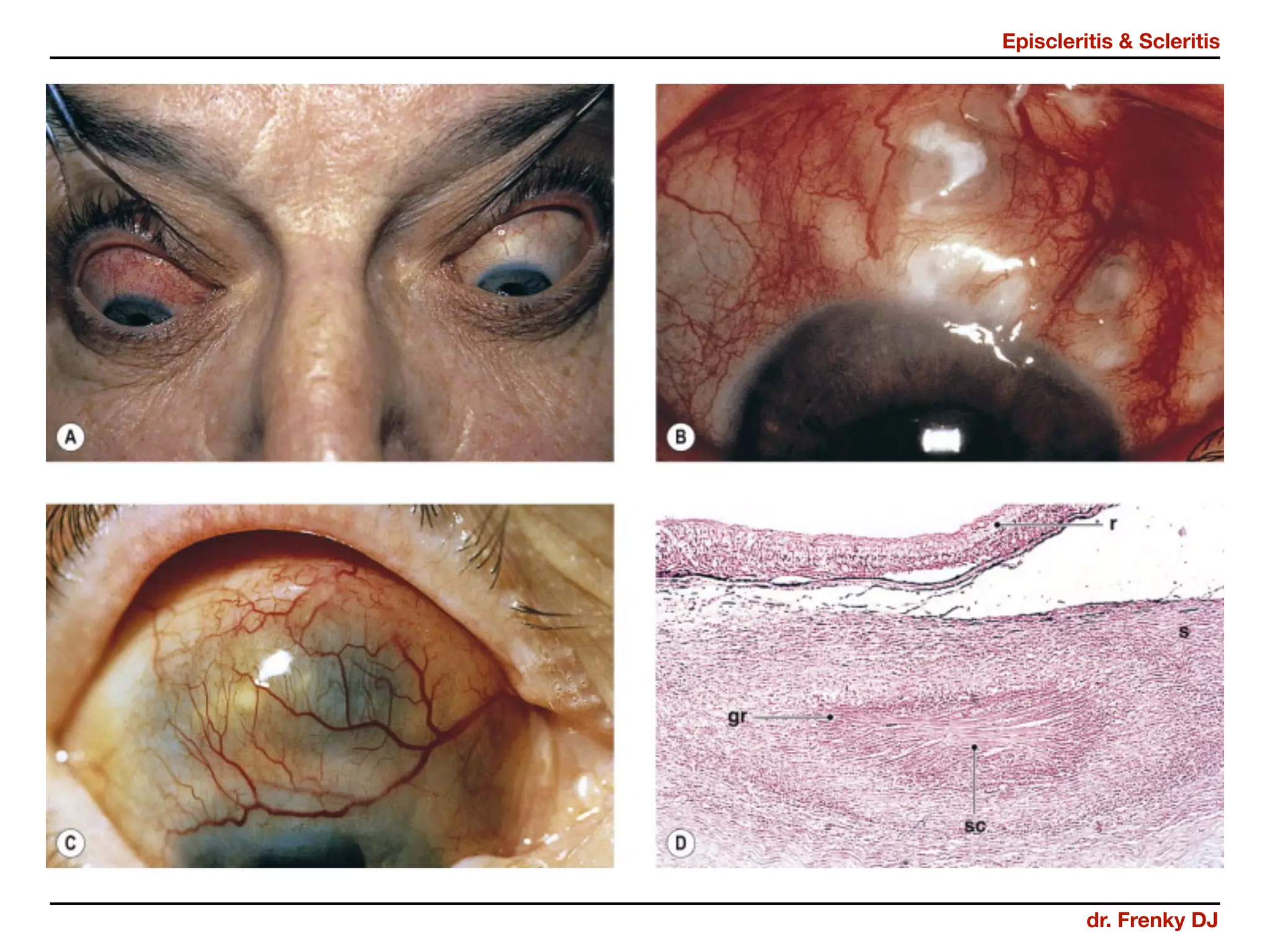
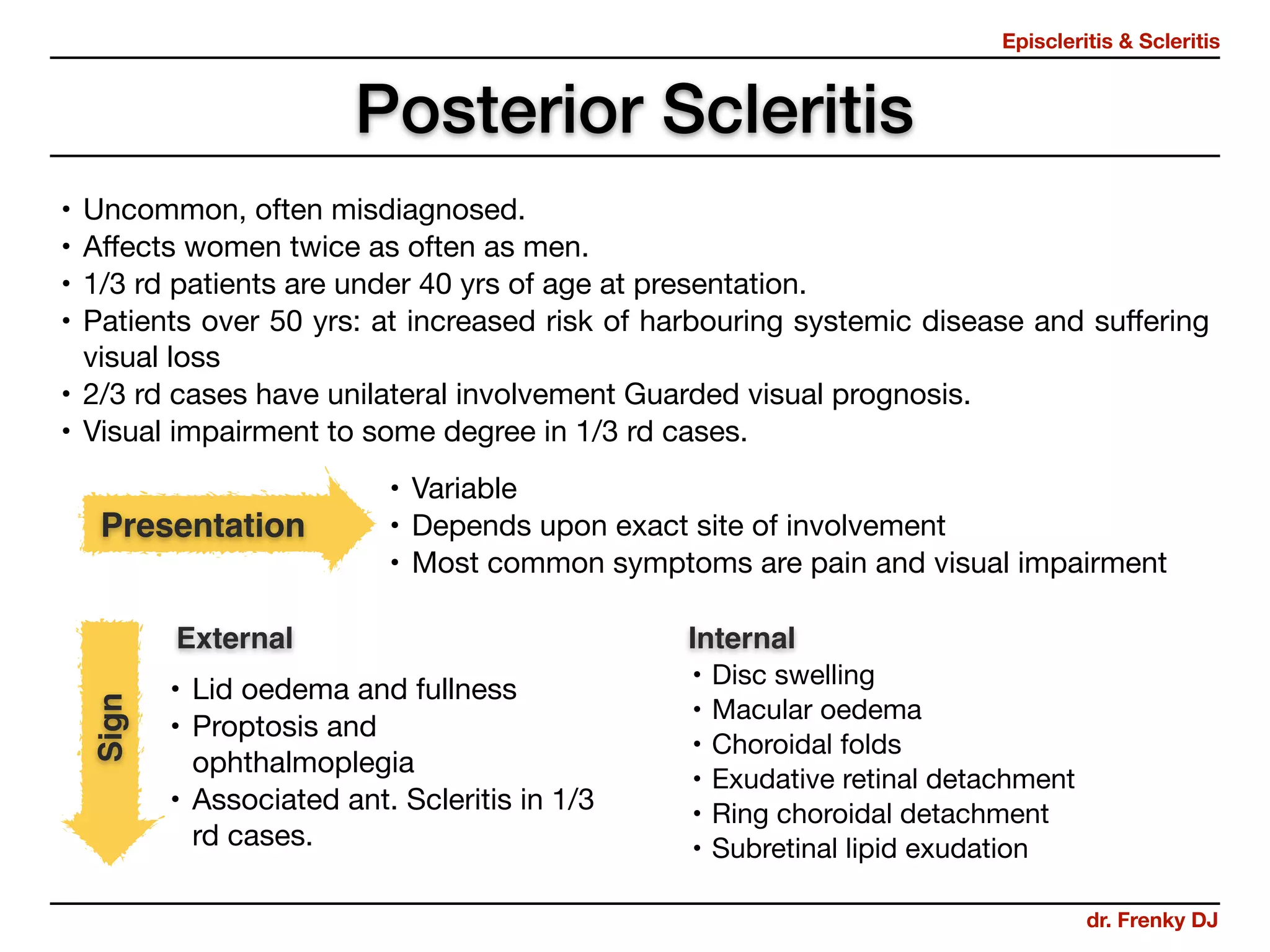




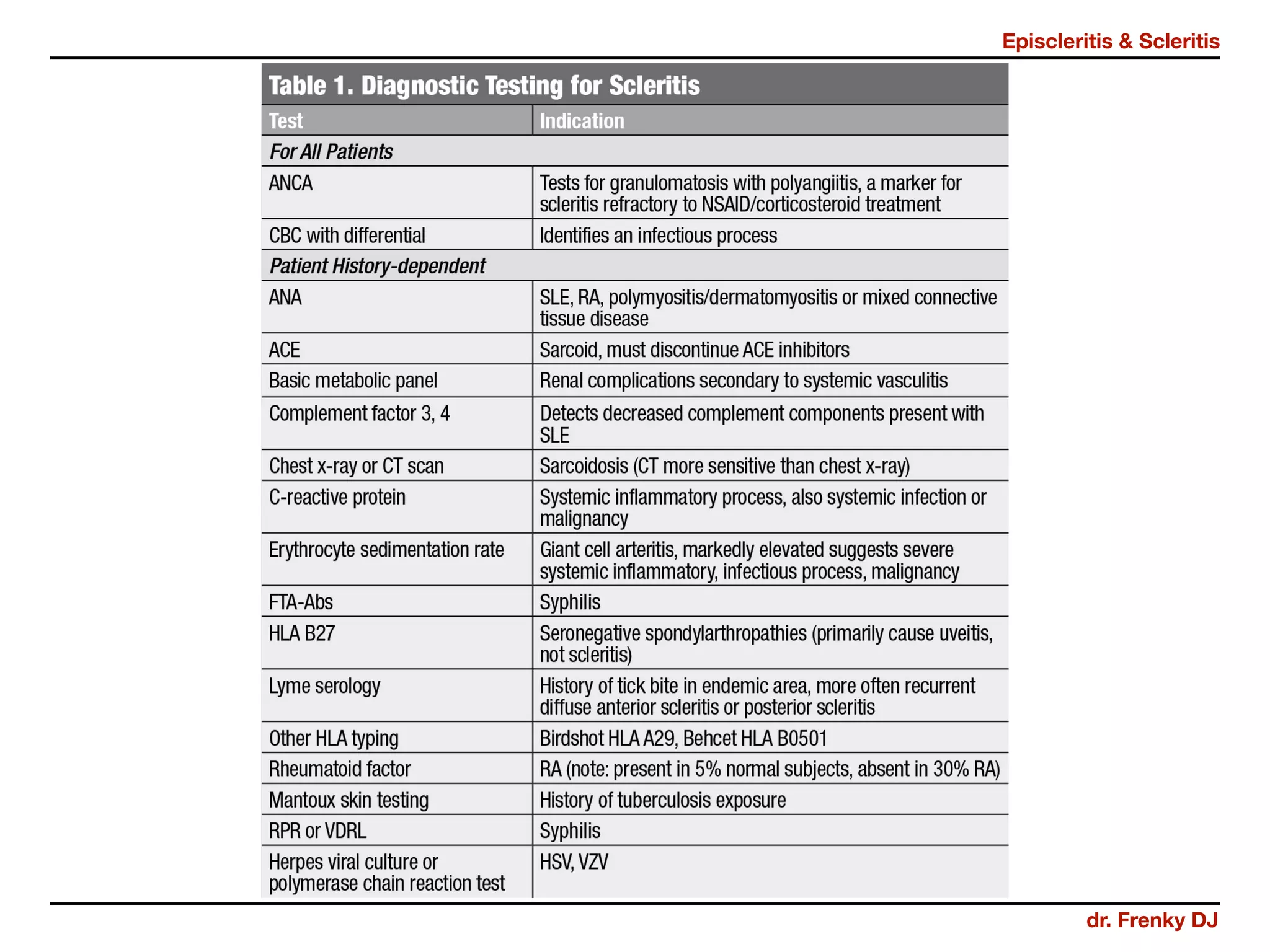




This document discusses episcleritis and scleritis. It defines episcleritis as an inflammatory condition affecting the episcleral tissue between the conjunctiva and sclera. Scleritis is characterized by edema and cellular infiltration of the scleral and episcleral tissues. The document classifies episcleritis and scleritis, describes their signs and symptoms, potential causes, diagnostic testing, and treatment options which may include topical or systemic corticosteroids and immunosuppressive medications. Complications are also outlined.











































































