Downloaded 1,429 times
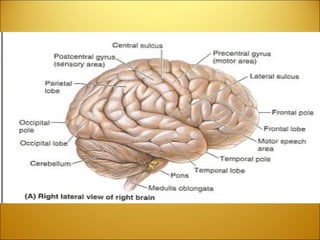
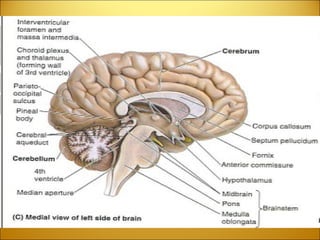
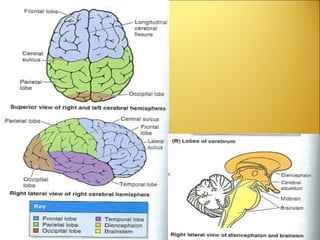
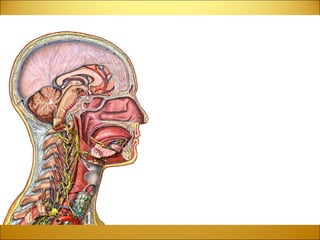

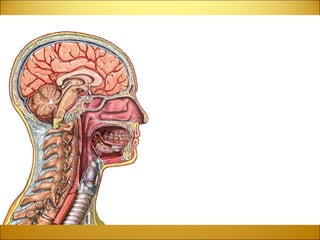
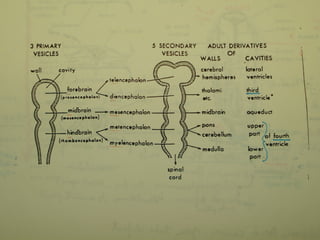
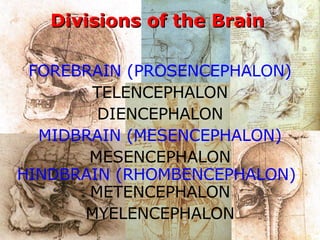

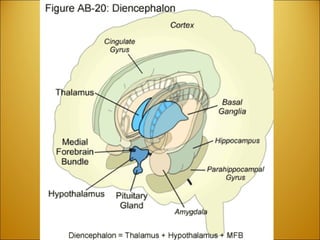

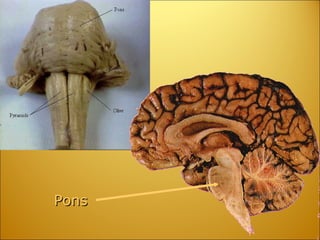
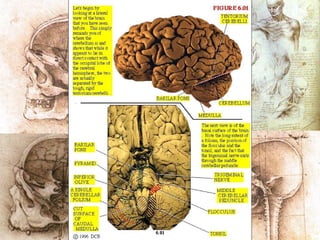

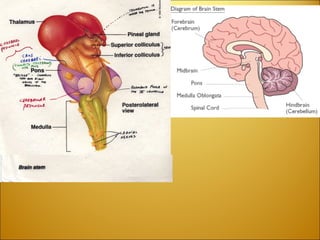
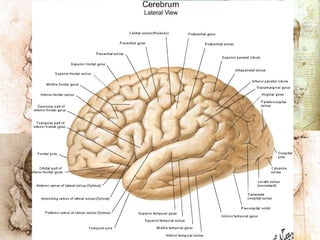
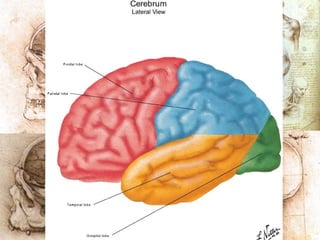
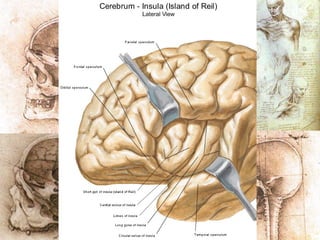
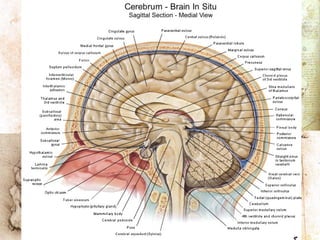
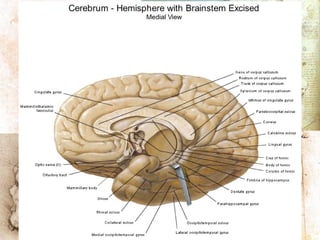
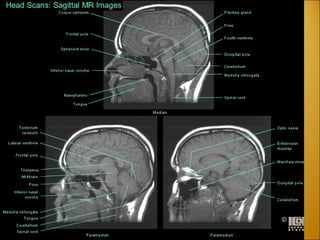
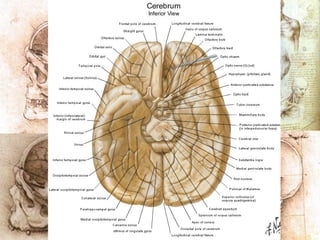
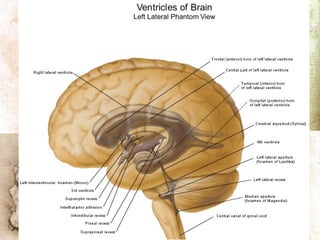
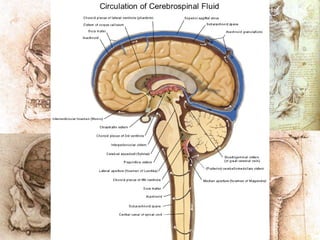
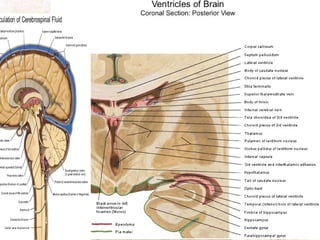
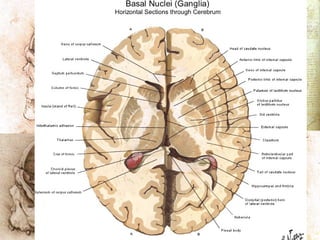
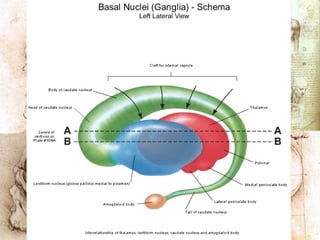
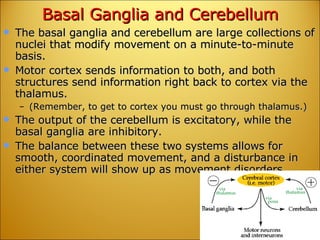
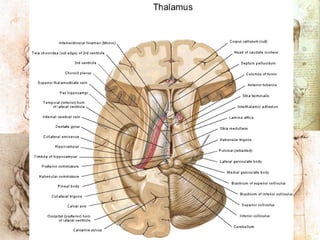
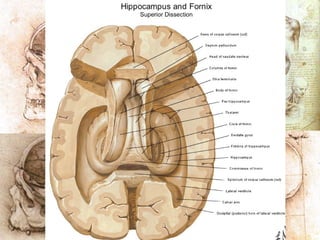
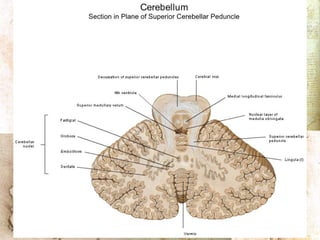
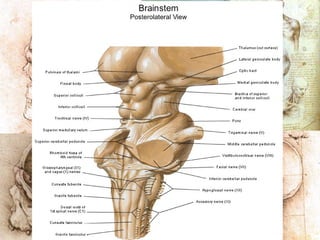
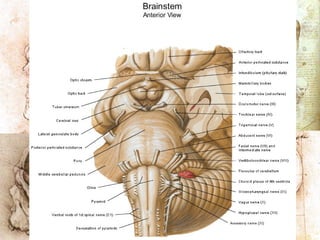
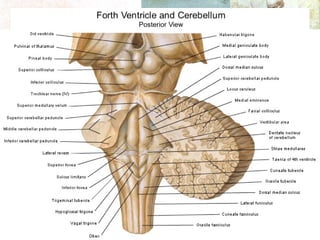
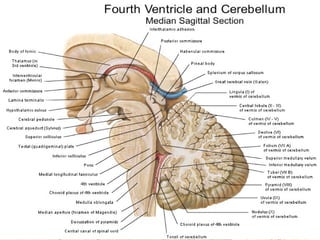
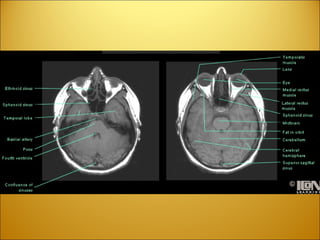
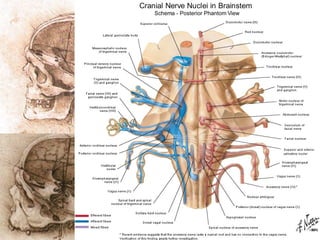
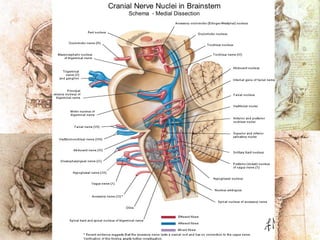
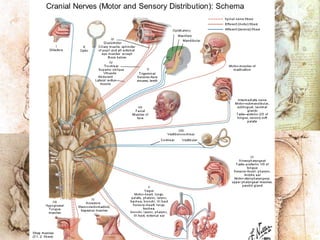
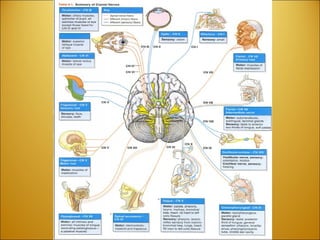
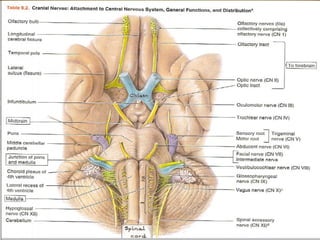




The document provides an overview of the divisions and structures of the brain, including the forebrain (telencephalon and diencephalon), midbrain, and hindbrain (metencephalon and myelencephalon). Key structures discussed include the cerebral hemispheres, thalamus, hypothalamus, pons, cerebellum, and medulla oblongata. Common neurological conditions like headaches, stroke, and Horner's syndrome are also briefly mentioned.











































































































