Downloaded 161 times

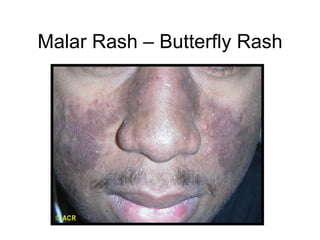
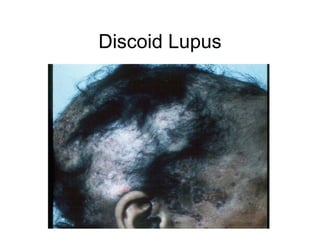

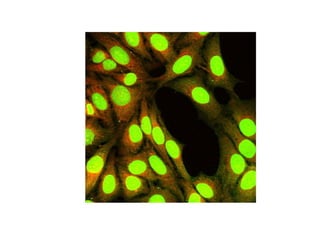
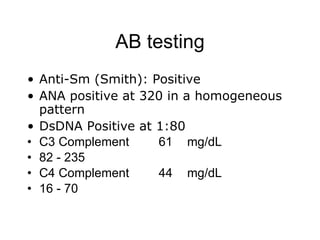

A 22-year-old college student presents with symptoms including a malar rash, photosensitivity, arthritis, fatigue, and hair loss. Laboratory tests show a positive ANA, positive anti-Smith antibody, and low white blood cell and platelet counts. This constellation of clinical features and laboratory results makes systemic lupus erythematosus the most likely diagnosis for the patient.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)