Downloaded 721 times


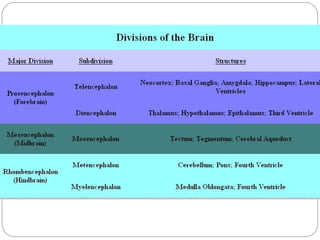
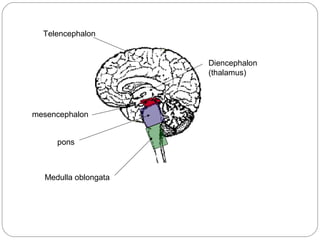

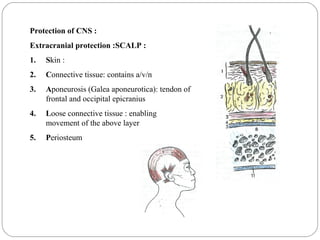







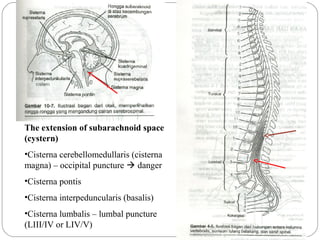



























This document provides an overview of clinically relevant neuroanatomy and outlines a problem-based learning approach. It discusses the central nervous system including structures like the brain, spinal cord, ventricles, and meninges. It also covers topics like cerebrospinal fluid circulation, blood vessel anatomy, motor and sensory pathways, and clinical conditions that can result from injuries to different parts of the nervous system like hemorrhages, paralysis, and more. The goal is to help students understand neuroanatomy concepts essential for medical cases through self-study materials and discussion of examples.