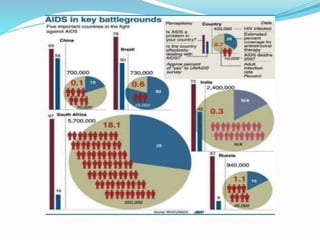
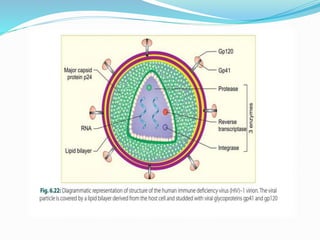
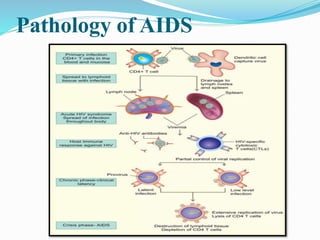
This document provides an overview of AIDS (Acquired Immunodeficiency Syndrome). It begins with an introduction defining AIDS as being caused by HIV. It then discusses the epidemiology, finding that as of 2017 approximately 36.9 million people globally are infected with HIV. It explores the etiology of AIDS, explaining that it is caused by the human immunodeficiency virus HIV. The document outlines the structure of HIV and its routes of transmission including sexual contact, intravenous drug use, and mother-to-child transmission. It describes the pathogenesis and life cycle of HIV, how it infects cells and integrates into the host cell genome. The document concludes with sections on symptoms, risk factors, diagnosis and management of AIDS.






















































.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/liverautosaved1-220330204054-thumbnail.jpg?width=640&height=640&fit=bounds)






















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





