The nervous system controls and coordinates the activities of the body. It has both voluntary and involuntary functions. The autonomic nervous system regulates involuntary functions like heart rate and digestion. It has two divisions - the sympathetic and parasympathetic systems which generally have opposing effects on organs. The sympathetic system prepares the body for fight or flight while the parasympathetic maintains normal functions. Dysfunctions of the autonomic nervous system can cause issues like high blood pressure, digestive problems, and more.
Blood supply of head & neck. Arterial & venous anastomosesEneutron
1. The coomon carotid artery
a) topography
- carotid sinus
- carotid body
2. Neurovascular bundles of the neck
3. The external carotid artery
4. The internal carotid artery
- arterial supply of the brain
5. Arterial anastomoses head and neck
6. Veins of the head and neck
Blood supply of head & neck. Arterial & venous anastomosesEneutron
1. The coomon carotid artery
a) topography
- carotid sinus
- carotid body
2. Neurovascular bundles of the neck
3. The external carotid artery
4. The internal carotid artery
- arterial supply of the brain
5. Arterial anastomoses head and neck
6. Veins of the head and neck
THE NEUROLOGICAL SYSTEM : CEREBROVASCULAR DISORDERSSeraGold
An overview of cerebrovascular disorders is given in this file, which includes ailments including aneurysms, strokes, and vascular abnormalities that affect the blood arteries in the brain. With a focus on causes, symptoms, diagnosis techniques, and treatment options, it provides a thorough overview of these important neurological diseases.
Unit IV -
Peripheral nervous system
Classification of peripheral nervous system: Structure and functions of
sympathetic and parasympathetic nervous system.
Origin and functions of spinal and cranial nerves.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
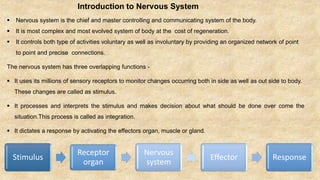
1. Introduction to Nervous System
Nervous system is the chief and master controlling and communicating system of the body.
It is most complex and most evolved system of body at the cost of regeneration.
It controls both type of activities voluntary as well as involuntary by providing an organized network of point
to point and precise connections.
The nervous system has three overlapping functions -
It uses its millions of sensory receptors to monitor changes occurring both in side as well as out side to body.
These changes are called as stimulus.
It processes and interprets the stimulus and makes decision about what should be done over come the
situation.This process is called as integration.
It dictates a response by activating the effectors organ, muscle or gland.
Stimulus
Receptor
organ
Nervous
system
Effector Response
2. Embryological Development of Nervous System:
Development of the nervous system in weeks 4 and 5 of the embryonic period. (a).Cross section of the neural tube,
the future spinal cord and brain. (b). Neuroblasts (future neurons) arise through division of neuroepithelial cells and
migrate externally. (c). Neuroblasts from the alar plate (future interneurons) and basal plate (future motor neurons).
4. Nervous
system
PNS
Cranial neves
and Spinal
nerves.
Sensory
[Afferent]
Division .
Somatic sensory
General
Touch,Pain,Pressure,Vibration,Temperature and
proprioception in skin and body wall.
Special - Vision,Smell,Hearing,Equilibrium.
Visceral sensory
General
Stretch,Pain,Temperature,Chemicalchanges and
irritation in viscera,nausea and hunger.
Special - Taste .
Motor
[Efferent]
Division.
Somatic motor
General- motor innervation of all skeletal muscles
[except pharyngeal arch muscles ]
Visceral motor
General
Motor innervation of smooth muscle ,cardiac
muscle,and glands ,equal to automnomic nervous
system[ANS].
Special- Motor innervation of pharyngeal arch muscles.
.
CNS
Brain and
Spinal cord .
6. Introduction to the Autonomic Nervous
system :
The ANS is the system of motor neurons that innervate
the smooth muscle, cardiac muscle, and glands of the
body. By controlling these effectors, the ANS regulates
such visceral funtions as heart rate, blood pressure,
digestion, and urination. These functions are essential for
maintaining the stability of the body's internal
environment. The ANS is the general visceral motor
division of the peripheral nervous system, according to
the classification of nervous outputs the ANS is distinct
from the general somatic motor division (Which
innervates the somatic skeletal muscles) and the special
visceral motor division (which innervates the pharyngeal
arch muscles).
7. Divisions of the Autonomic
Nervous System :
The ANS has two divisions, the
sympathetic and parasympathetic. Both
divisions generally innervate the same
visceral organs, but cause opposite
effects: Where one division stimulates
some smooth muscle to contract or a
gland to secrete, the other division
inhibits that action.
8. The Parasympathetic Division
The cranial part of the parasympathetic division innervates organs in the head, neck, thorax, and most of the
abdomen.The sacral part supplies the rest of the abdominal organs and the pelvic organs.
Cranial Outflow
The cranial parasympathetic outflow is
contained in several cranial nerves. More
specifically, the preganglionic fibers run in
the oculomotor, facial, glossopharyngeal,
and vagus nerves.
9. Oculomotor Nerve (III)
The parasympathetic fibers of the oculomotor nerve
innervate smooth muscles in the eye that cause the
pupil to constrict and the lens of the eye to bulge
actions that allow focusing on close objects in the
field of vision.
Facial Nerve (VII)
The parasympathetic fibers of the facial nerve stimulate the
secretion of many glands in the head, including two salivary
glands inferior to the mouth, called the submandibular and
sublingual glands; the lacrimal (tear) gland above the eye;
and mucus-secreting glands in the nasal cavity.
10. Glossopharyngeal Nerve (IX)
The parasympathetic fibers of the glossopharyngeal
nerve stimulate secretion of a large salivary gland
called the parotid gland, which lies anterior to the ear.
Vagus Nerve (X)
Parasympathetic fibers from one additional cranial
nerve, the vagus nerve, innervate the visceral organs of
the thorax and most of the abdomen.
11. The sacral part of the parasympathetic
outflow comes from the S2–S4 segments of
the sacral spinal cord (Figure 14.3). It
supplies the organs in the pelvis, including
the distal half of the large intestine, the
bladder, the reproductive organs (the
uterus, for example), and the erectile
tissues of the external genitalia.
Parasympathetic effects on these organs
include stimulation of defecation, voiding of
urine, and erection
Sacral Outflow
12. The Sympathetic Division
The sympathetic division is more complex than the parasympathetic division, in part because it innervates more
organs. It supplies not only all the visceral organs in the internal body cavities but also -all visceral structures in
the superficial regions of the body: the sweat glands, the hair-raising arrector pili muscles of the skin, and the
smooth musculature in the walls of arteries and veins.
SYMPATHETIC GANGLIA
Chain or
paravertebral
ganglia
Many chain ganglia line up vertically
along both sides of the vertebral
column, from the neck to the pelvis.
Successive chain ganglia are
interconnected by short nerves into
long sympathetic trunks. Each
sympathetic trunk resembles a strand
of beads. There is approximately one
chain ganglion for each spinal nerve.
Pre vertebral or
collateral
ganglia
They are not paired and are not
segmentally arranged. they are confined
to the abdomen and pelvis and they all
lie anterior to the vertebral column
mostly on the abdominal aorta. The
main prevertebral ganglia are the celiac,
superior mesenteric, inferior mesenteric,
and inferior hypogastric ganglia.
14. Characteristic Sympathetic Parasympathetic
Origin Thoracolumbar outflow: lateral horn of gray matter of spinal cord
segments T,-L2
Craniosacral outflow: brain stem nuclei of cranial nerves
III,VII,IX,andX;spinalcordsegmentsS2-S4
Locationofganglia Ganglia within afewcmofCNS:alongside vertebralcolumn
(paravertebralganglia) and anteriorto vertebralcolumn
(prevertebral ganglia)
Ganglia in or close to visceral organ served
Relative length of pre- and postganglionic fibers Rami
communicantes
Shortpreganglionic; longpostganglionic Long preganglionic; short postganglionic
Degreeofbranchingofpreganglionicfibers Extensive Minimal
Functionalgoal Prepares body tocope withemergenciesand intense muscular
activity
Maintenance functions;conservesand storesenergy
Neurotransmitters Allpreganglionicfibersrelease ACh mostpostganglionicfibers
release norepinephrine (adrenergicfibers)somepostganglionic
fibers(e.g.,thoseservingsweat glands and bloodvesselsofskeletal
muscles)release ACh,neurotransmitteractivity augmented by
release ofadrenal medullaryhormones(norepinephrine and
epinephrine)
All fibersrelease ACh (cholinergicfibers)
15. Target organ Sympatheticeffects Parasympathetic effects
Eye (iris) Stimulatesdilatormuscles,dilateseye pupils Stimulates constrictor muscles; constricts eye pupils
Eye (ciliarymuscle) No effect Stimulates muscles, which results in bulging of the lens for accommodation and
close vision
Glands(nasal,lacrimal,salivary,gastric,pancreas) Inhibitssecretoryactivity;causesvasoconstriction of blood vessels supplying the glands Stimulatessecretoryactivity
Sweatglands Stimulatescopioussweating(cholinergicfibers) No effect
Adrenal medulla Stimulatesmedullacellstosecreteepinephrineandnoreppinephrine No effect
Arrector pili muscles attachedto hair follicles Stimulatestocontract(erectshairsandproducesgooseburmps0 No effect
Heart muscle Increasesrateandforceofheartbeat Decreasesrate slows andsteadiesheart
Heart: coronary blood vessels Causesvasodilation Constrictscoronaryvessels
Bladder/ urethra Causesrelaxationofsmoothmuscleofbladderwallconstrictsurethralspphincterinhibitsvoiding Causes contraction of smooth muscle of bladder wall; relaxes urethral sphincter;
promotesvoiding
Lungs Dilatesbronchiolesandmildlyconstrictsblood vessels Constrictsbronchioles
Digestive tract organs Decreases activity of glands and muscles of digestive system and constricts sphincters (e.g., anal
sphincter)
Increases motility (peristalsis) and amount of secretion by digestive organs; relaxes
sphinctersto allowmovementof foodstuffsalong tract
Gallbladder Inhibits(gallbladderisrelaxed) Excites(gallbladdercontractstoexpelbile)
Kidney Causesvasoconstictiondecreasesurineoutput Noeffect
Penis Causesejaculation Causeserection(vasodilation)
Vagina/clitoris Causesreverseperistalsis(contraction)ofvagina Causeserection(vasodilation)ofclitoris
Blood Vessels Constricts most vessels and increases blood pressure; constricts vessels of abdominal viscera
and skin to divert blood to muscles, brain, and heart when necessary; dilates vessels of the
skeletal muscles (cholinergic fibers)duringexercise
Littleorno effect
Blood coagulation Increasescoagulation Noeffect
Cellular metabolism Increasesmetabolicrate Noeffect
Adipose tissue Stimulateslipolysis(fatbreakdown) Noeffect
16. Pathways to the Body Periphery
The vagus nerve, the autonomic nerve plexuses, and the autonomic ganglia throughout the body. All
autonomic plexuses are shared by both parasympathetic and sympathetic fibers, but the ganglia in these plexuses are
almost exclusively sympathetic. Also note the sympathetic chain ganglia.
17. Sympathetic pathways
This diagram indicates the relationship of the
sympathetic neurons to the spinal cord, sympathetic
trunks, and associated structures. Preganglionic
neurons in the spinal cord, labeled a—c, send fibers to
the chain ganglia. There, these fibers may synapse with
a postganglionic neuron in a chain ganglion (neuron a)
or may pass through to synapse in a prevertebral
ganglion (neuron c). Also, a preganglionic fiber may
ascend or descend in the sympathetic trunk (neuron b)
before synapsing in a chain or prevertebral ganglion.
19. Central Control of the Autonomic Nervous System
Although the ANS is not considered to be under direct voluntary control, its performance is nevertheless
regulated by the central nervous system.
Control by the Brain Stem and Spinal Cord
The reticular formation of the brain stem appears to exert the most direct influence over autonomic functions.
Centers in the medulla oblongata regulate heart rate (cardiac center), the diameter of blood vessels (vasomotor
center), many types of digestive activities (vomiting center), and respiration rate (respiratory centers).Control of
autonomic functions at the level of the spinal cord involves the spinal visceral reflexes.
Control by the Hypothalamus
The integration center of the autonomic nervous system is the hypothalamus. These hypothalamic centers exert
their effects indirectly via relays through the reticular formation. It is through the ANS that the hypothalamus
controls heart activity, blood pressure, body temperature, and digestive functions.
Control by the Cerebral Cortex
People can learn to control some autonomic functions indirectly by developing extraordinary control over their
emotions. For example, feelings of extreme calm are associated with parasympathetic activation.
20. Referred Pain
People suffering from visceral pain often perceive this
pain as somatic in origin—as if it originated from the skin
or outer body. This is called referred pain. For example,
heart attacks can produce pain in the superior thoracic
wall and the medial aspect of the left arm. The cause of
referred pain is not fully understood. However, it is
known that both the affected organ and the region of
the body wall to which the pain is referred are
innervated by the same spinal segments. (For
example, both the heart and the skin area to which
heart pain projects are innervated by sensory neurons
from T1 to T5) The current view is that damage to the
visceral organ causes painful, reflexive vasoconstriction
in the corresponding somatic segments.
21. Pathology of the Autonomic Nervous System
Since the ANS is involved in nearly every important process that occurs within the body, it is not surprising that
abnormalities of autonomic functioning can have far-reaching effects. Such abnormalities can impair blood
delivery and elimination processes and can threaten life itself.
Raynaud's disease is characterized by intermittent
attacks, during which the skin of the fingers and toes
becomes pale, then blue and painful. The severity of this
disease ranges from mere discomfort to such extreme
constriction of vessels that gangrene (tissue death)
results. Raynaud's disease is treated with drugs that
inhibit vasoconstriction. In severe cases, however,
cutting the preganglionic sympathetic fibers serving the
affected region is necessary. The involved vessels then
dilate, reestablishing adequate blood delivery.
22. Hypertension, or high blood pressure, can result from overactive sympathetic vasoconstriction promoted
by continual stress. Hypertension is always serious because (1) it increases the work load on the heart,
possibly precipitating heart disease and (2) it increases the wear and tear on the artery walls. Stress-induced
hypertension is treated with drugs that prevent the muscle cells in the walls of blood vessels from binding
with norepinephrine and epinephrine.
Achalasia of the cardia is a condition in which the
esophagus loses its ability to propel swallowed food
inferiorly. Additionally, the smooth muscle surrounding the
inferior end of the esophagus (cardiac sphincter) contracts
to block the passage of food into the stomach (achalasth
means "failure to relax"). Accumulating food stretches the
esophagus to enormous width, and meals cannot be kept
down. This condition usually appears in young adults and is
thought to result from an insufficient number of
parasympathetic postganglionic neurons in the esophagus
wall.
23. Congenital megacolon or Hirschsprung's
disease is a birth defect in which the parasympathetic
innervation of the distal region of the large intestine fails to
develop normally. Feces accumulate proximal to the
immobile bowel segment, greatly distending this area
(megacolon = enlarged large intestine). The condition is
corrected surgically by removing the inactive part of the
infant's intestine.