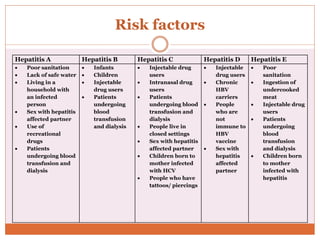
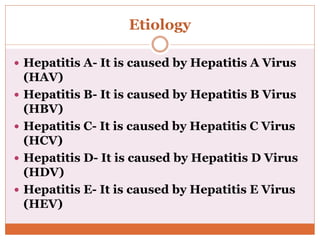
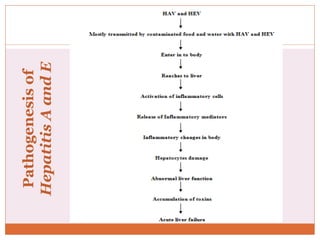
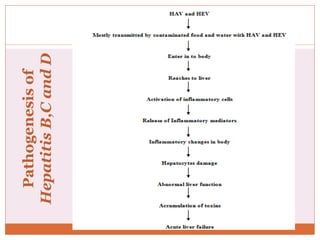
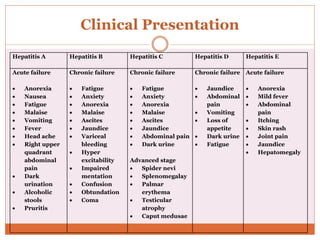
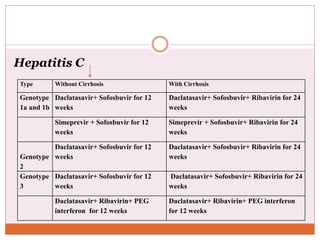
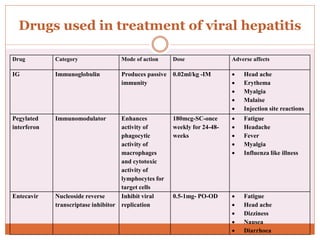
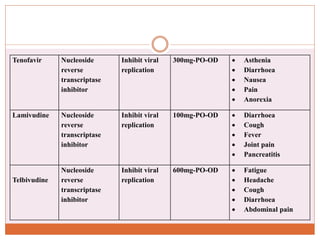
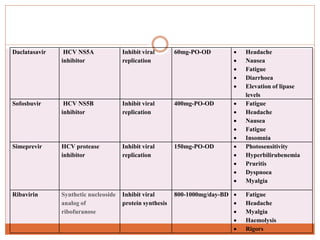
This document discusses viral hepatitis, which causes liver inflammation and damage from hepatitis viruses A-E. It provides details on the epidemiology, types, risk factors, pathogenesis, clinical presentation, complications, diagnosis, treatment and drugs used for each viral hepatitis type. Globally over 2 billion people are infected with hepatitis viruses resulting in over 1 million deaths annually. In India, chronic hepatitis B and C infections account for 40-50% and 12-32% of liver cancer cases, respectively. Treatment involves vaccination, antiviral drugs like interferons, immunoglobulins and symptomatic care depending on the viral type and disease stage.