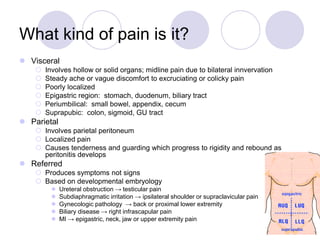
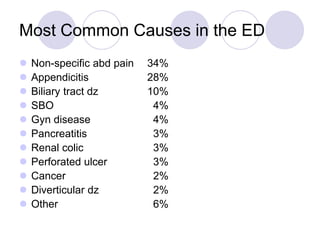
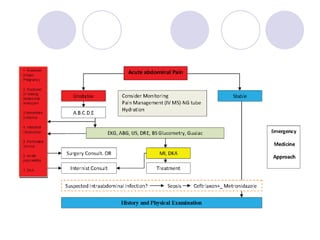
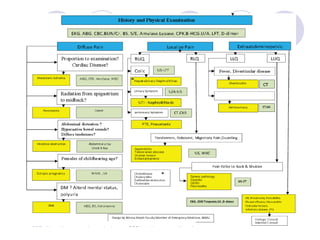
The document discusses a case of acute abdominal pain in a 24-year-old male. It provides details of the patient's history, physical exam findings, and differential diagnosis. The document then reviews approaches to evaluating abdominal pain, including types of pain, history taking, physical exam maneuvers, potential diagnoses, appropriate tests, and disposition planning.