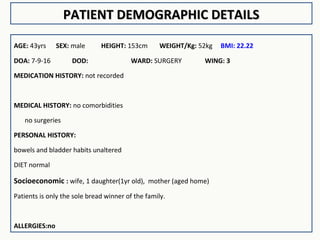
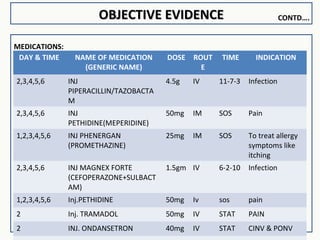
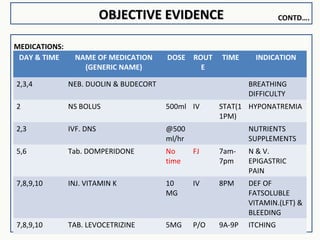
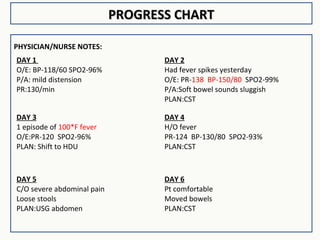
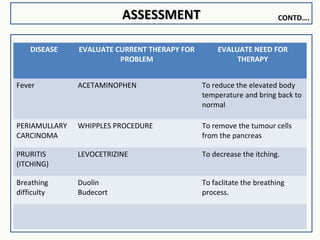
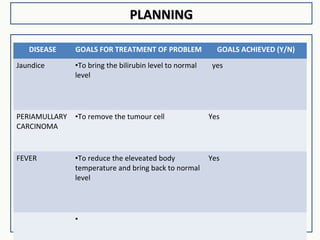
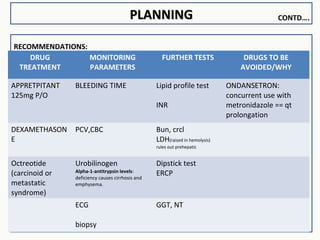
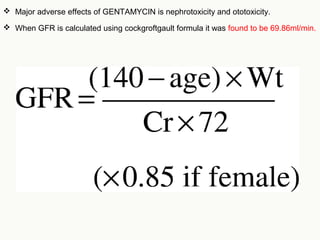
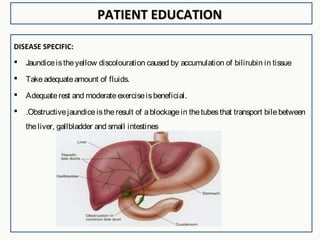
The document provides a case presentation on obstructive jaundice in a 43-year-old male patient. It includes demographic details, medical history, subjective and objective evidence from examinations and lab reports, medications, progress notes, assessments, care plan, pharmacist interventions, and patient education. The assessments determined the patient had obstructive jaundice likely due to periampullary carcinoma. Treatment included antibiotics, analgesics, vitamins, and surgery to remove the tumor, with the goals of reducing fever, itching, and jaundice which were achieved.


























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














