Download to read offline
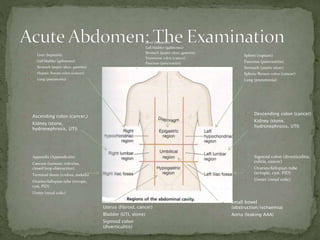





This document provides an overview of the causes, differential diagnosis, history and exam findings, investigations, and management of acute abdominal pain. It lists potential causes by organ system and describes typical symptoms and signs. Common etiologies include appendicitis, diverticulitis, colorectal cancer, bowel obstructions, and perforations. The examination involves inspection, palpation for tenderness and masses, percussion, and auscultation of bowel sounds. Basic investigations include blood tests, urine analysis, imaging like CXR and CT. Management focuses on ABCs, IV fluids, analgesia, antibiotics, and supportive care, with urgent surgery for generalized peritonitis, perforation, or irreducible hernias.























































