Downloaded 11 times



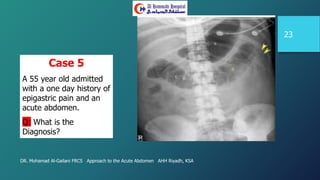
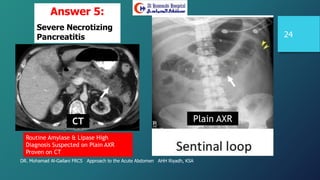




This document discusses the approach to acute abdominal pain, emphasizing the distinction between benign and serious conditions, and the need for urgent surgical intervention in life-threatening cases. It highlights the significant number of emergency admissions for abdominal pain and stresses the importance of experienced surgeons in triaging cases effectively. The document also outlines key symptoms, signs, diagnostic investigations, and pre-operative optimization strategies to improve patient outcomes.





















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

