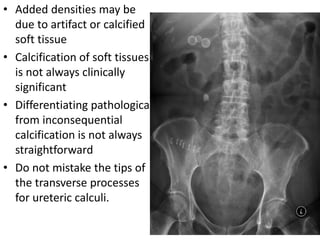
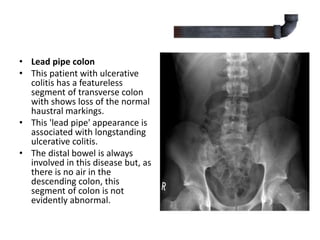
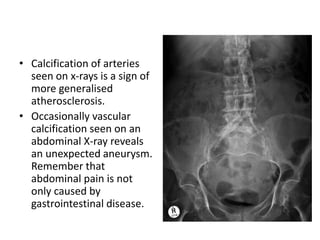
- The document discusses the technical aspects and normal findings of abdominal radiography for non-traumatic emergencies. It outlines how to assess radiographs and what normal structures should be seen, including the bones, organs and bowel gas patterns. Common abnormal findings are also reviewed such as pneumoperitoneum which can indicate a perforated viscus. A list of non-traumatic abdominal emergencies that may present with acute abdominal pain is provided.



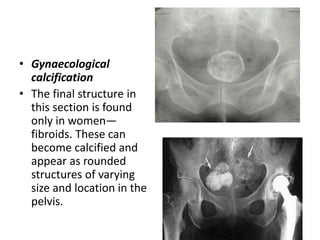




















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





