X-Ray Reading
1. Plain/ Contrast
2. View or Orientation
3. Part of body
4. Systematic examination (ABCDE)
4.
ABCDE
• A -A is for Air in the wrong place
Look for pneumoperitoneum & pneumoretroperitoneum
Look for gas in the biliary tree and portal vein
• B - B is for Bowel
Look for dilated small and large bowel
Look for a volvulus
Look for a distended stomach
Look for a hernia
Look for evidence of bowel wall thickening
5.
ABCDE
• C -C is for Calcification
Look for clinically significant calcified structures such as
renal calculus, nephrocalcinosis, pancreatic calcification and
an abdominal aortic aneurysm (AAA), calcified gallstones
Look for clinically insignificant calcified structures such as
costal cartilage calcification, phleboliths, mesenteric lymph
nodes, calcified fibroids, prostate calcification and vascular
calcification
Look for a foetus (females)
6.
ABCDE
• D -D is for Disability (bones and solid organs)
Look at the bony skeleton for fractures and sclerotic/lytic bone
lesions
Look at the spine for vertebral body height, alignment, pedicles and
a ‘bamboo spine’
Look for solid organ enlargement
• E - E is for Everything else
Look for evidence of previous surgery and other medical devices
Look for foreign bodies
Look at the lung bases
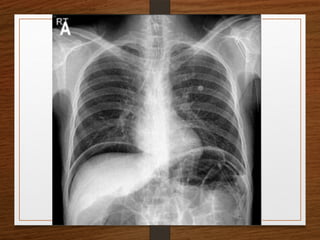
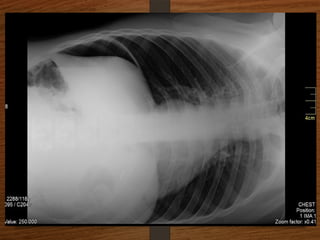
PNEUMOPERITONEUM
• Miss itand the patient may die
• Bilateral dark crescents of gas under both domes of diaphragm
• Erect posture
• Left lateral decubitus
• 1 ml of air is more than enough
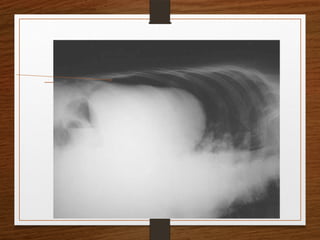
15.
Signs of pneumoperitoneum
•Double wall sign ( RIGLER’S sign )
• Football sign – centrally placed intraperitoneal free air
• Dome sign
• Cupola sign of air under the central diaphragm
• Silver’s sign – visualization of falciform ligament
• Continuous diaphragm sign
• Lucent liver sign – air overlying or outlining liver
• Doges cap sign – triangle of air outlinig morrison’s
pouch
• Inverted V sign - air in umbilical ligaments
16.
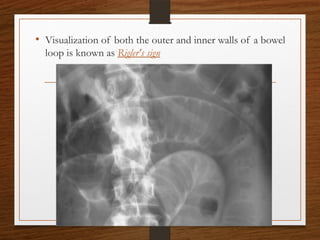
• Visualization ofboth the outer and inner walls of a bowel
loop is known as Rigler's sign
17.
Causes of pneumoperitoneum
Withperitonitis
Perforation of a hollow viscus , peptic ulcer most often
Intestinal obstruction
Ruptured diverticular disease
Penetrating injury – gun shot , knife wounds
Ruptured inflammatory bowel disease(megacolon)
Colonic infections (typhoid)
18.
Causes of pneumoperitoneum
Withoutperitonitis
Post laparotomy
Post laparoscopy
Jejunal diverticulosis
Steroids
Tracking from chest (pneumothorax)
Peritoneal dialysis
Vaginal insufflation (douching, hysteroscopy)
Pneumatosis coli
19.
Conditions mimicking pneumoperitoneum
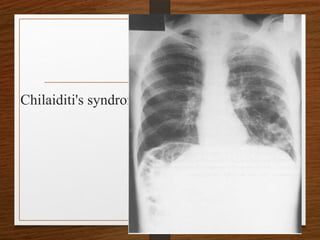
Intestinebetween liver and diaphragm—Chilaiditi's
syndrome
Subphrenic abscess
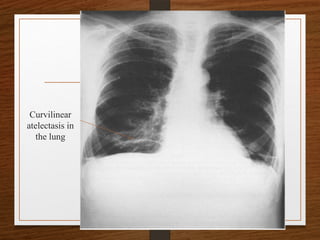
Curvilinear atelectasis in the lung
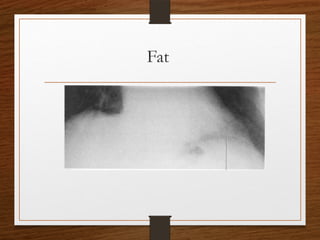
Subdiaphragmatic fat
Diaphragmatic irregularity
Cysts in pneumatosis intestinalis
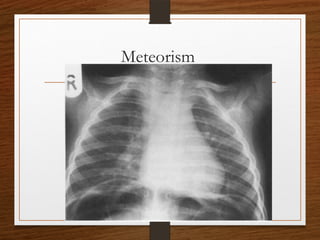
Meteorism
Distended gastric fundus
Peptic Ulcer Perforation
•Aetiology
• Clinical features
• Stages
• Investigation
• Management
• Resuscitation
• Surgery
26.
• Fluid levelsare common in normal people, and they
usually lie in the colon.
• Three to five fluid levels less than 2.5 cm in length may
be seen, particularly in the right lower quadrant, without
any evidence of intestinal obstruction or paralytic ileus.
• More than two fluid levels in dilated small bowel (calibre
greater than 2.5 cm) are said to be abnormal, and
usually indicate
• Paralytic ileus or
• Intestinal obstruction
27.
• The causesof SBO are myriad, but can be largely divided into
• Mural lesions
• tumour,
• stricture due to Crohn's disease,
• irradiation,
• ischaemia
• Luminal
• bezoar,
• gallstone,
• Ascaris lumbricoides bolus,
• intussusception
• Extrinsic
• adhesions,
• hernia,
• volvulus,
• abdominal malignancy
28.
Distinction between small-and large-bowel
dilatation
• Dilated small-bowel loops are usually more numerous and arranged centrally in
the abdomen.
• The loops show a small radius of curvature and rarely exceed 5 cm in diameter.
• The presence of solid faeces is the only reliable sign that the loop is large
bowel. The other signs can be misleading.
• The small-bowel folds or valvulae conniventes form thin, complete bands across
the bowel gas shadow, prominent in the jejunum but becoming less marked as
the ileum is reached.
• The valvulae conniventes are much closer together than colonic haustra and
become thinner when stretched.
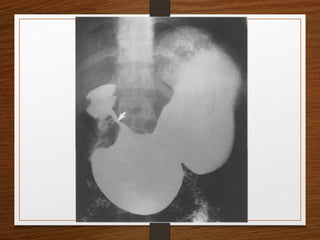
30.
Sigmoid volvulus
The invertedU-shaped loop is usually massively distended
Commonly devoid of haustra, an important diagnostic point.
The ahaustral margin can often be identified overlapping respectively
the lower border of the liver shadow (the liver overlap sign),
the haustrated, dilated descending colon (the left flank overlap sign)
the left side of the pelvis (the pelvic overlap sign).
The top of the sigmoid volvulus usually lies very high in the abdomen
(above the level of T10) with its apex on the left side.
31.
Signs
Grossly distendedloop of sigmoid colon
Coffee bean sign
Air – fluid ratio > 2:1
Lack of haustra
Apex above 10th
thoracic vertebra
Liver overlap sign
Left flank overlap sign
Pelvis overlap sign
Bird of prey /twisted bird beak appearance
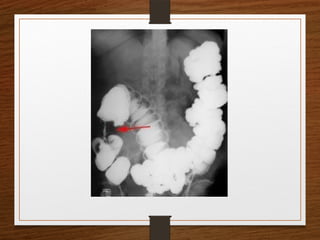
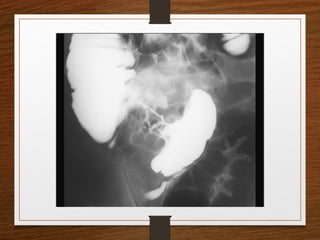
Contrast enema
• Featuresseen at the point of torsion include a
smooth, curved tapering of the colonic lumen, like a
hooked beak (the bird of prey sign)
• the mucosal folds often show a ‘screw’ pattern at the
point of twist
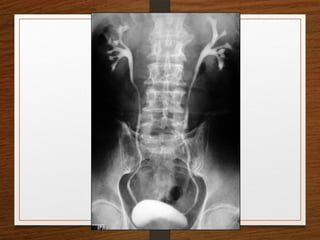
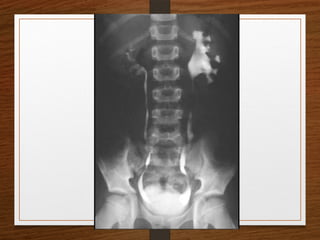
36.
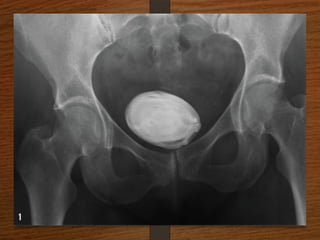
What are theD/D of a radiopaque shadow in this region?
• Kidney stone
• Gallstones
• Pancreatic calculi
• Foreign body
• Fecolith
• Phleboliths
• calcified lymph node
• calcified renal tuberculosis
• calcified adrenal gland
• chip fracture of a transverse process of vertebra or calcification of costal
cartilage
41.
What are theimportant causes of
cannon ball shadows in chest X-ray?
• Metastasis
• Benign lesion
Fungal infection—Histoplasmosis, coccidioodomycosis,
aspergillosis.
Parasitic infection—Filarial infection, hydatid disease.
Sarcoidosis.
Wegener’s granulomatosis.
Rheumatoid nodules.
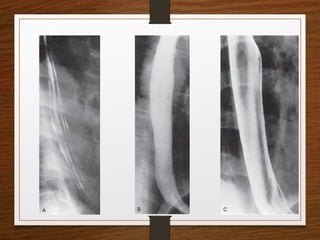
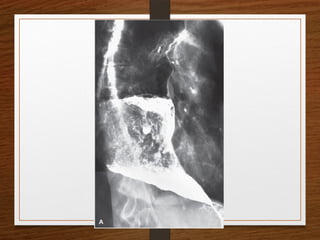
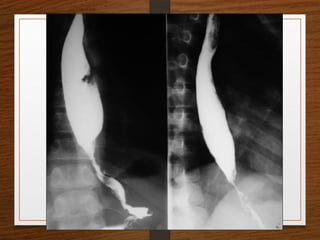
Barium Studies
Barium studiescan demonstrate GI abnormalities in three ways
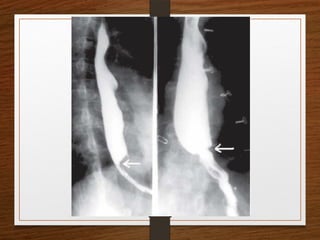
1. Mucosal relief views of the collapsed or partially collapsed
lumen obtained with a small volume of barium.
• particularly useful for showing abnormalities involving the
submucosa, such as esophageal varices.
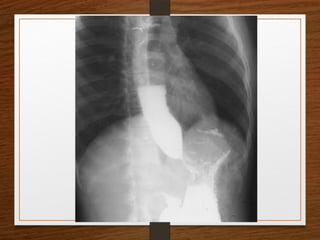
2. Single-contrast views of the filled lumen obtained with a
large volume of low-density barium
• These views enable visualization of contour abnormalities,
strictures, and large polypoid defects.
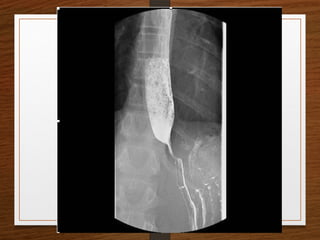
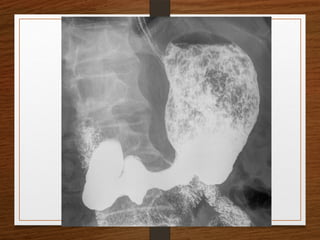
3. Double-contrast views obtained after the mucosal surface
has been coated with a thin layer of high-density barium
and the lumen has been distended with gas
• These views enable visualization of subtle mucosal lesions, such as
the early changes of inflammatory bowel disease and early
neoplastic lesions
44.
• Barium suspensionsfor single-contrast studies
should be of moderate density (50%-100% w/v)
when not diluted.
• For the double-contrast examination, we use high-
density 250% w/v barium