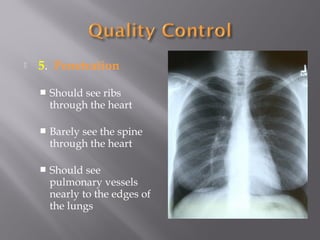
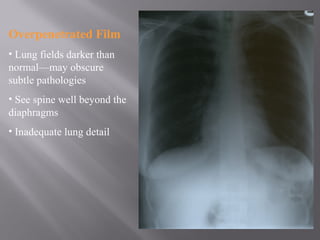
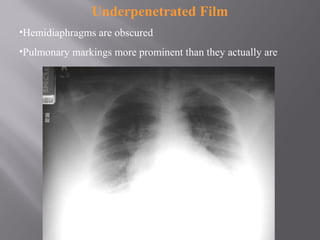
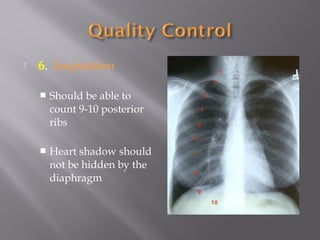
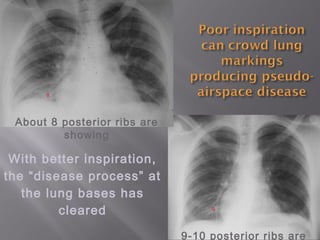
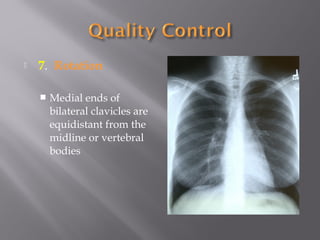
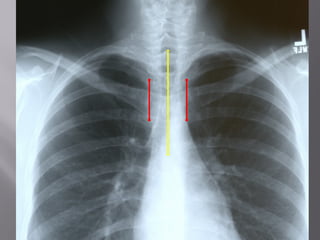
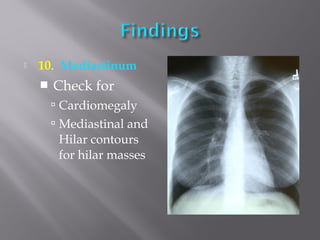
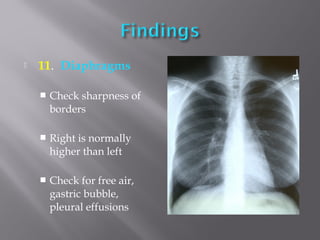
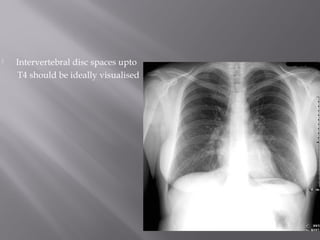
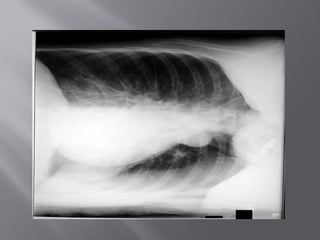
Chest x-rays are commonly used to examine the lungs but have limitations as they provide a 2D image of a 3D structure. It is important to follow proper protocol for chest x-ray imaging including checking patient details, film quality, inspiration level, and positioning. Key aspects of positioning involve ensuring proper centering, angles, and inspiration to obtain quality images and accurately interpret findings. Following standardized guidelines is vital for consistent and accurate chest x-ray interpretation.