The document discusses the ABO blood group system, including its discovery, genetics, biochemistry, antigens, antibodies, and implications for transfusion. Some key points:
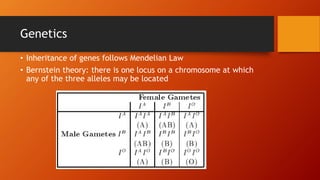
- Karl Landsteiner discovered the main ABO blood groups (A, B, AB, O) in 1900. The ABO blood type is determined by alleles at a single gene locus.
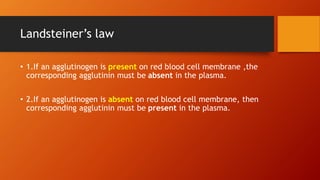
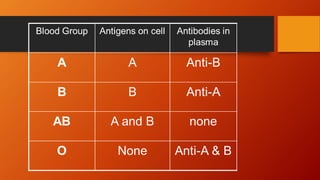
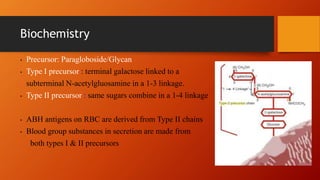
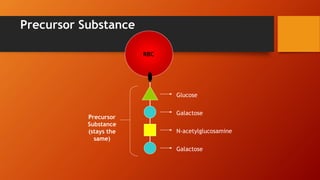
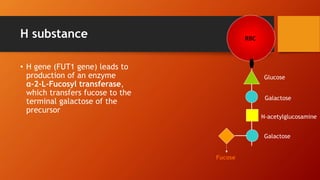
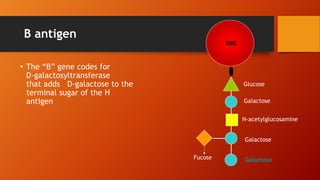
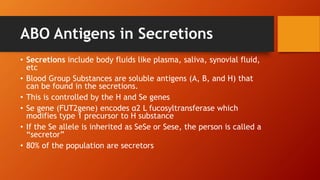
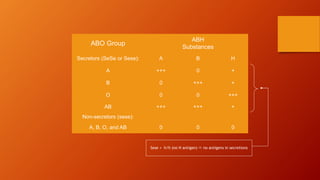
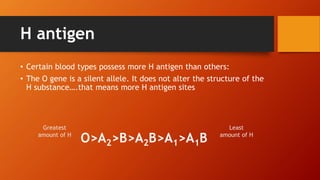
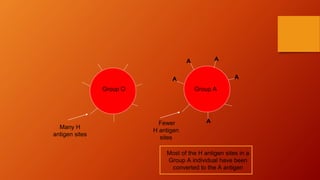
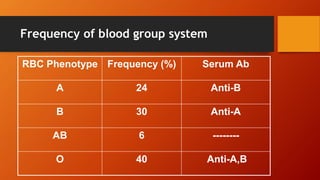
- The antigens are carbohydrate structures on red blood cells. People naturally produce antibodies against antigens they lack.
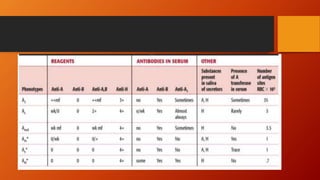
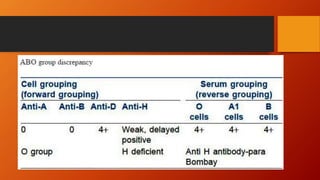
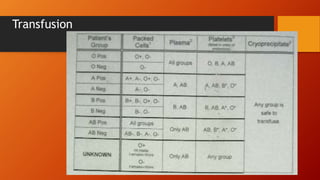
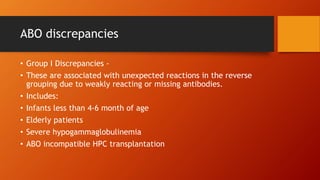
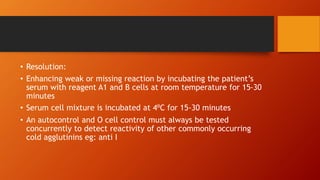
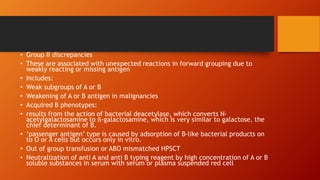
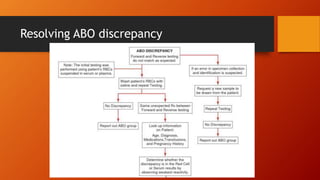
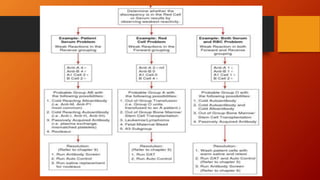
- ABO typing must be accurate to avoid transfusion reactions. Discrepancies can occur due to weak subgroups, diseases, or test issues. Resolving discrepancies helps ensure patient and donor safety.














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














