Downloaded 280 times

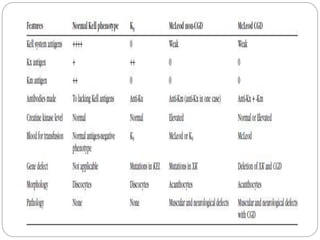
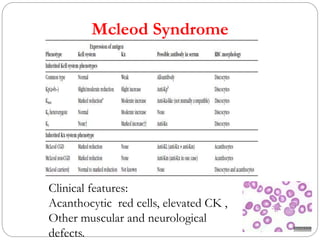

The document provides an overview of the Kell blood group system, detailing its history, nomenclature, antigens, antibodies, genetics, and clinical significance. It covers the characteristics of major Kell antigens, their prevalence across different populations, and the implications for transfusion medicine and hemolytic diseases. Additionally, it discusses the genetic complexities and phenotypes associated with the Kell system, including the clinical features of conditions like McLeod syndrome.










































![Blood group.007[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bloodgroup-140326055444-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)