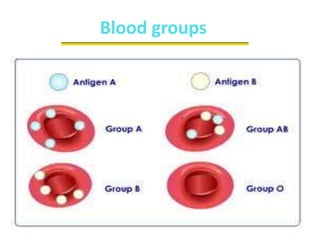
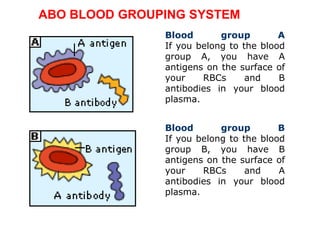
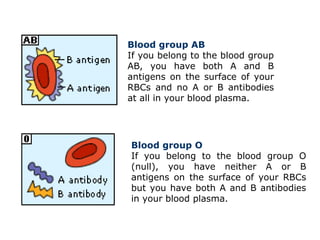
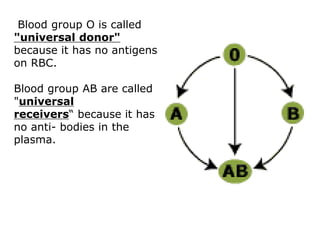
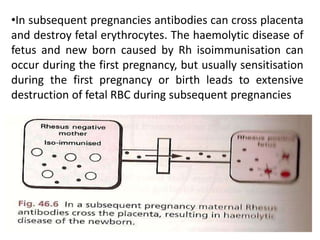
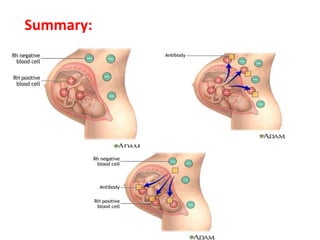
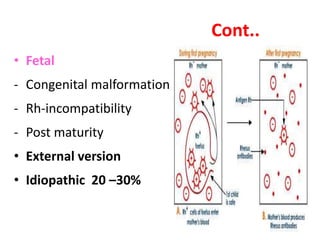
The document discusses isoimmune disease and Rh incompatibility. It defines isoimmune disease as an immune disease caused by antigens from another person. Rh incompatibility occurs when a mother is Rh-negative and the baby is Rh-positive, potentially causing hemolytic disease in the baby. The document outlines the major blood group systems, Rh factor, causes and pathogenesis of Rh incompatibility, methods of detection and treatment including intrauterine transfusions and exchange transfusions. It also discusses nursing management and risk factors for intrauterine fetal demise.



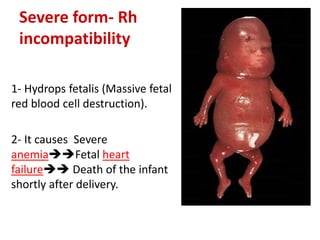














































![Blood group.007[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bloodgroup-140326055444-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

























































