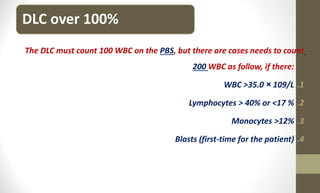
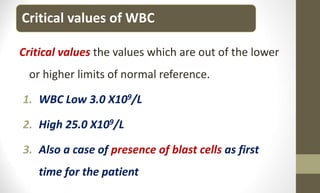
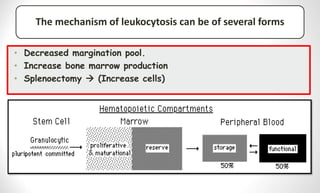
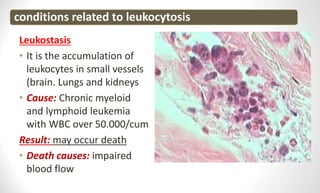
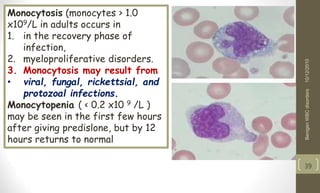
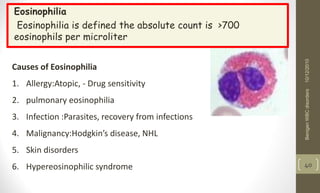
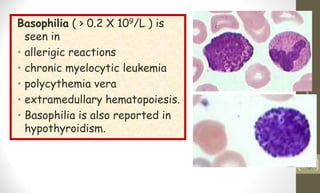
The document focuses on abnormalities in leukocyte numbers, detailing various types of white blood cell (WBC) abnormalities, including leukocytosis, leukopenia, and their mechanisms, causes, and classifications. It emphasizes the importance of absolute WBC counts over relative counts and discusses the significance of differential leukocyte counts for diagnosing conditions. Additionally, it highlights criteria and conditions associated with specific leukocyte types, and concludes with methods for evaluating and interpreting leukocyte abnormalities.