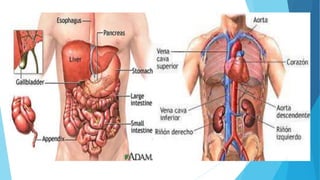
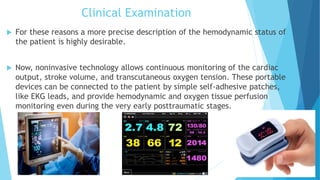
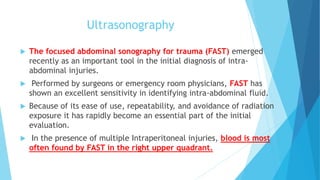
This document discusses the evaluation and management of abdominal injuries. It notes that abdominal injuries occur in 13% of trauma patients and are associated with a 7.7% mortality rate. Blunt trauma can cause organ lacerations and bleeding while penetrating trauma risks organ perforation. Clinical examination is important to assess for peritonitis and hemodynamic instability which indicate need for exploration. Focused abdominal sonography for trauma (FAST) can identify fluid but CT is preferred for stable patients. Diagnostic laparoscopy and laparotomy may be needed but have limitations in fully evaluating injuries.