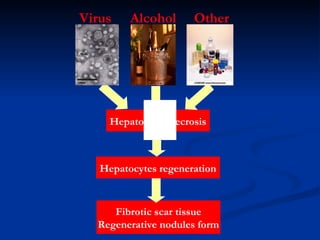
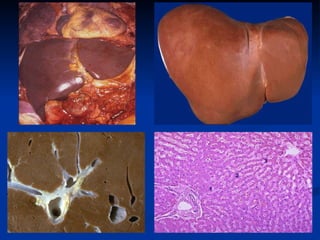
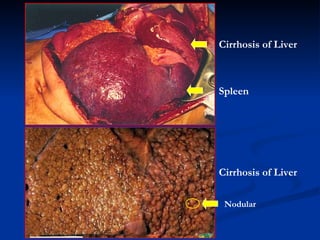
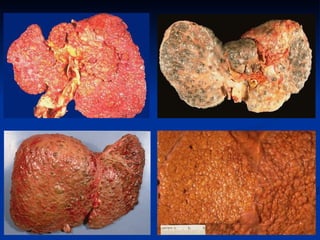
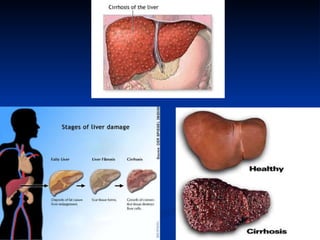
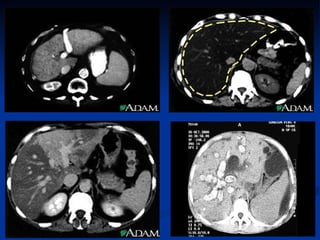
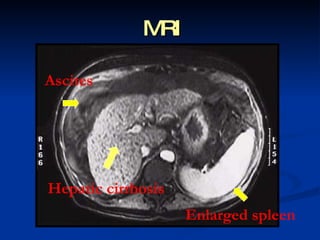
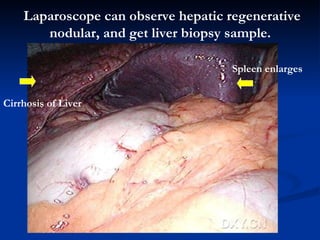
This document provides information about hepatic cirrhosis, including its definition, description, causes, risk factors, types, clinical manifestations, diagnosis, and complications. Specifically, it defines cirrhosis as scarring of the liver that reduces its function over time. Long-term alcohol use and chronic hepatitis B and C infections are major causes of cirrhosis worldwide. Clinical signs of cirrhosis include fatigue, abdominal pain, and jaundice. Complications arise when the liver decompensates and can no longer function properly, leading to issues like portal hypertension and ascites.