Downloaded 2,197 times


















![Investigations
Measurement of pancreatic products in blood
Enzymes
Pancreatic polypeptide II
Measurement of pancreatic exocrine secretion
Direct measurements
1. Enzymes
2. Bicarbonate
Indirect measurement
1. Bentiromide test
2. Schilling test
3. Fecal fat, chymotrypsin, or elastase concentration
4. [14C]-olein absorption](https://image.slidesharecdn.com/chronicpancreatitis-141031121633-conversion-gate01/75/Chronic-pancreatitis-19-2048.jpg)






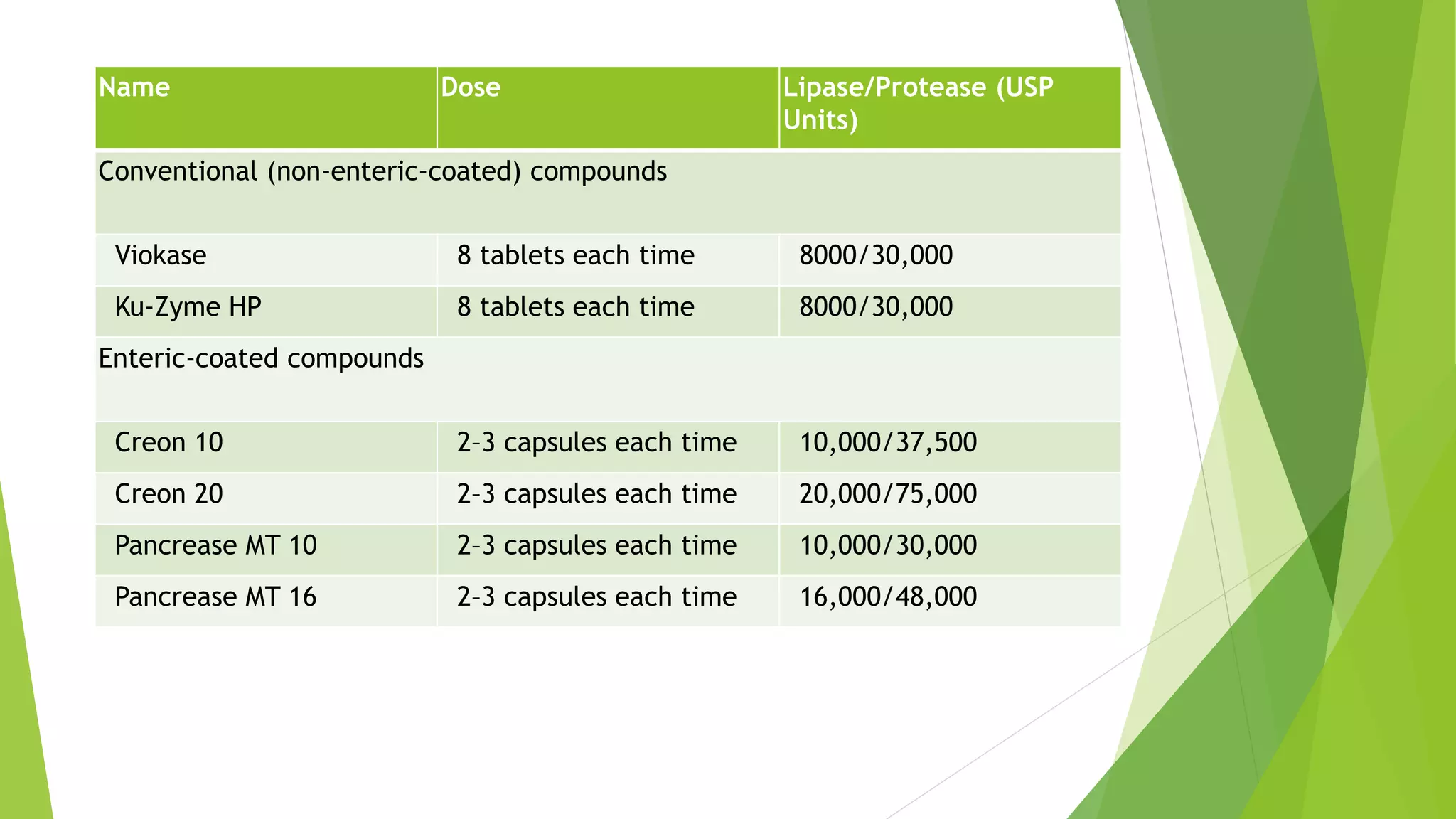

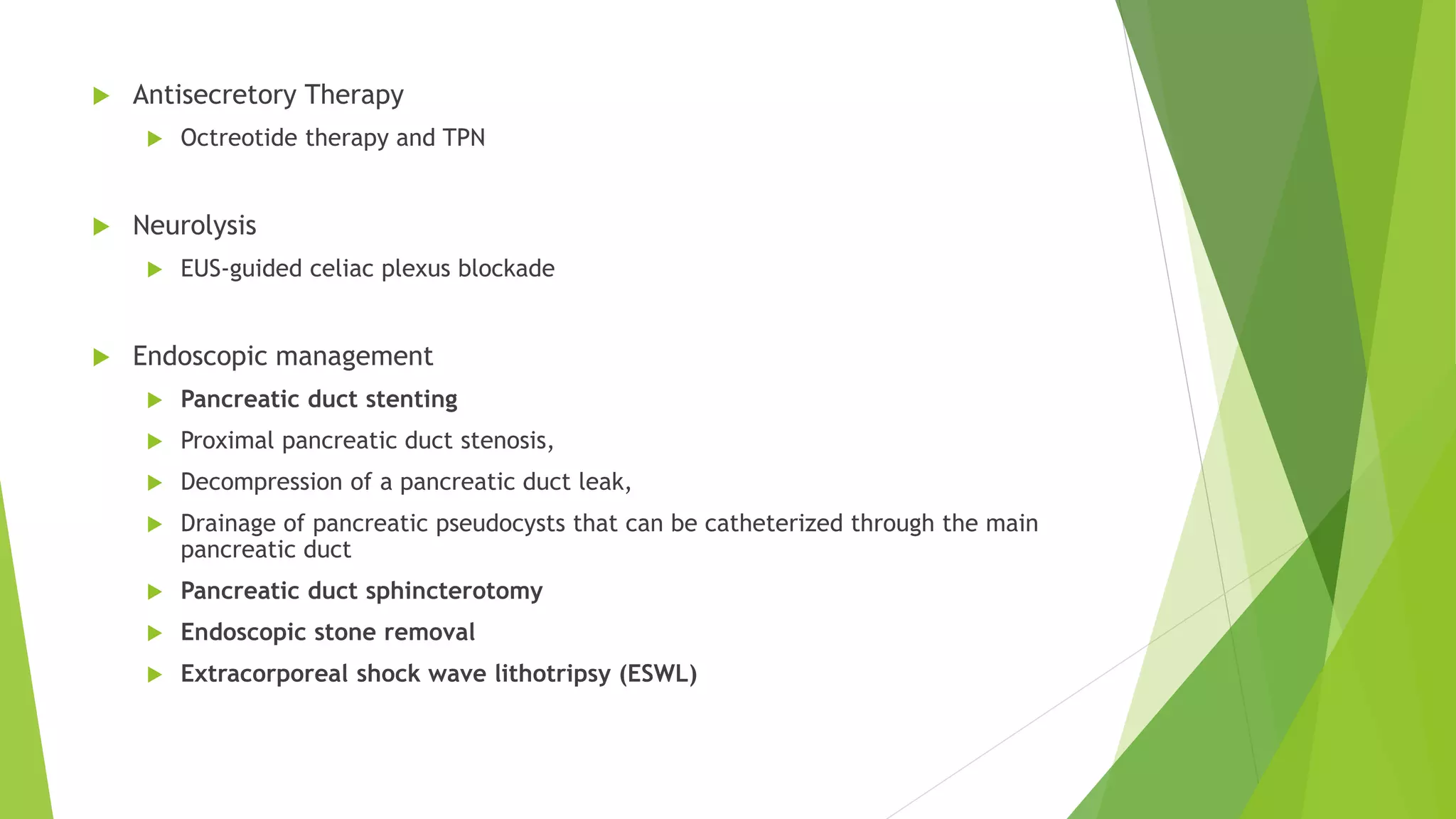



















Chronic pancreatitis is a chronic inflammatory condition of the pancreas characterized by progressive fibrosis of the pancreatic parenchyma and loss of function. It has multiple etiologies but alcohol use is the most common cause. Patients experience abdominal pain, steatorrhea from maldigestion, and can develop diabetes. Treatment involves pain management, pancreatic enzyme replacement, and in severe cases, surgery such as drainage procedures or pancreatic resections.

















































































