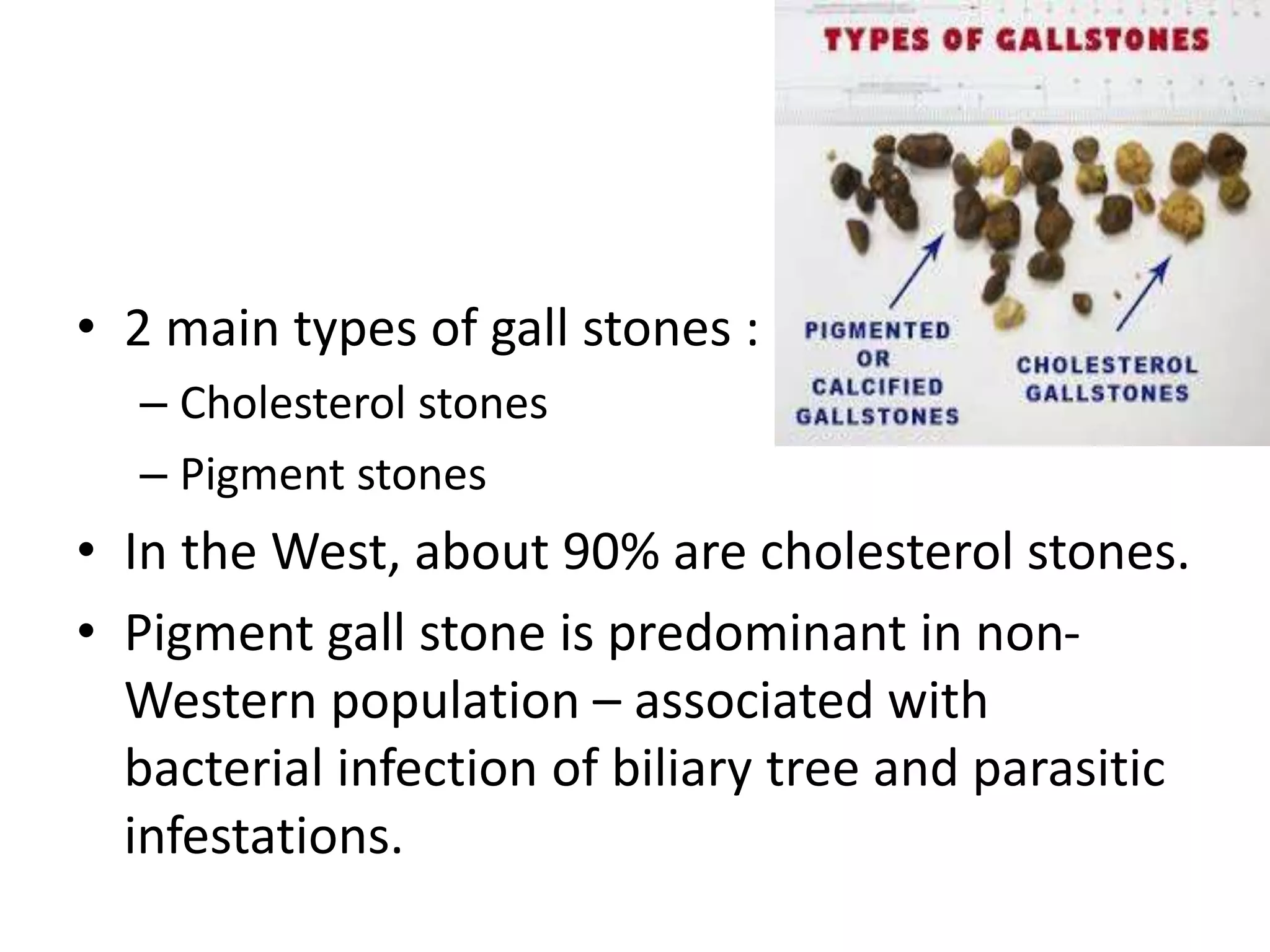
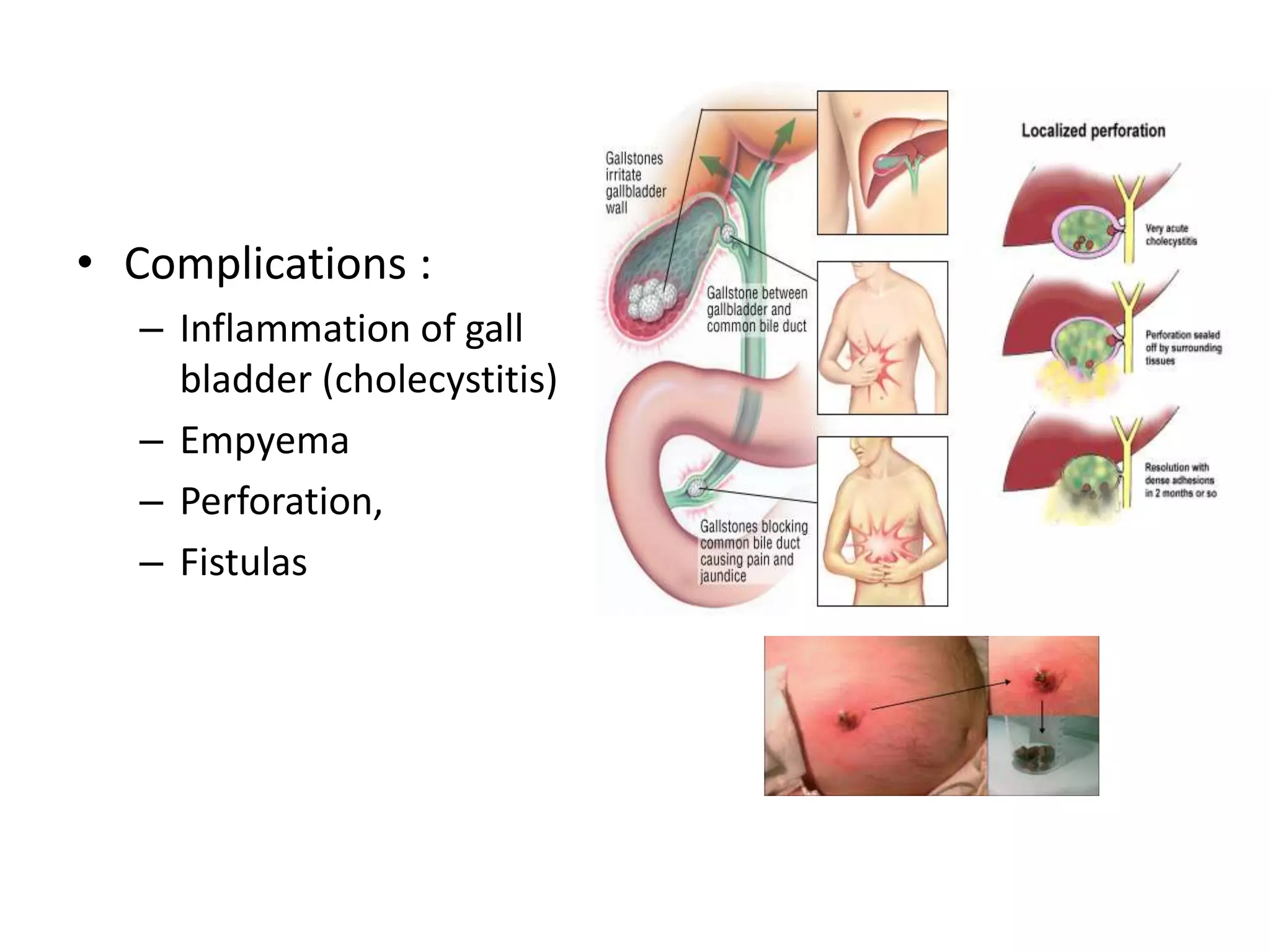
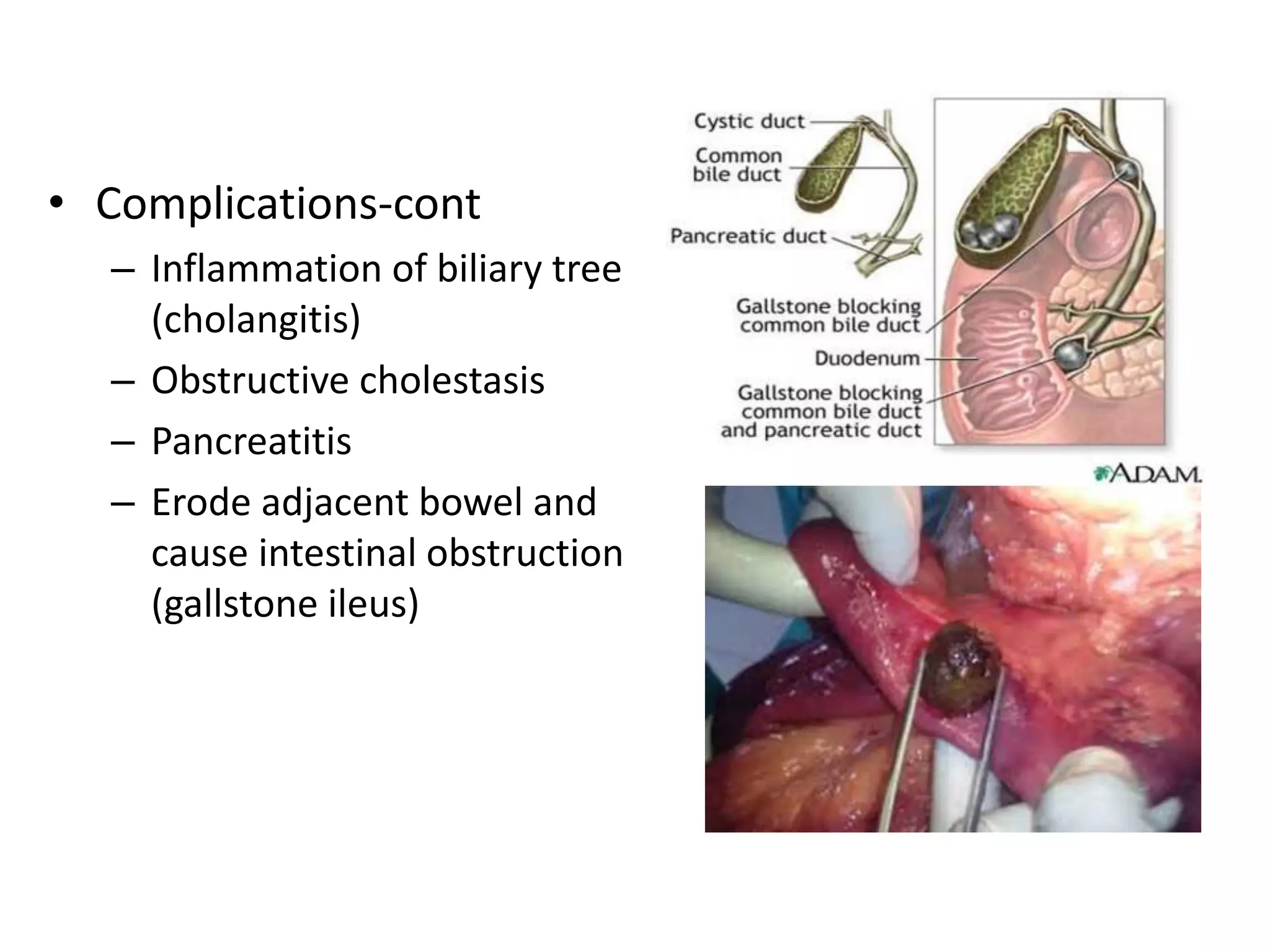
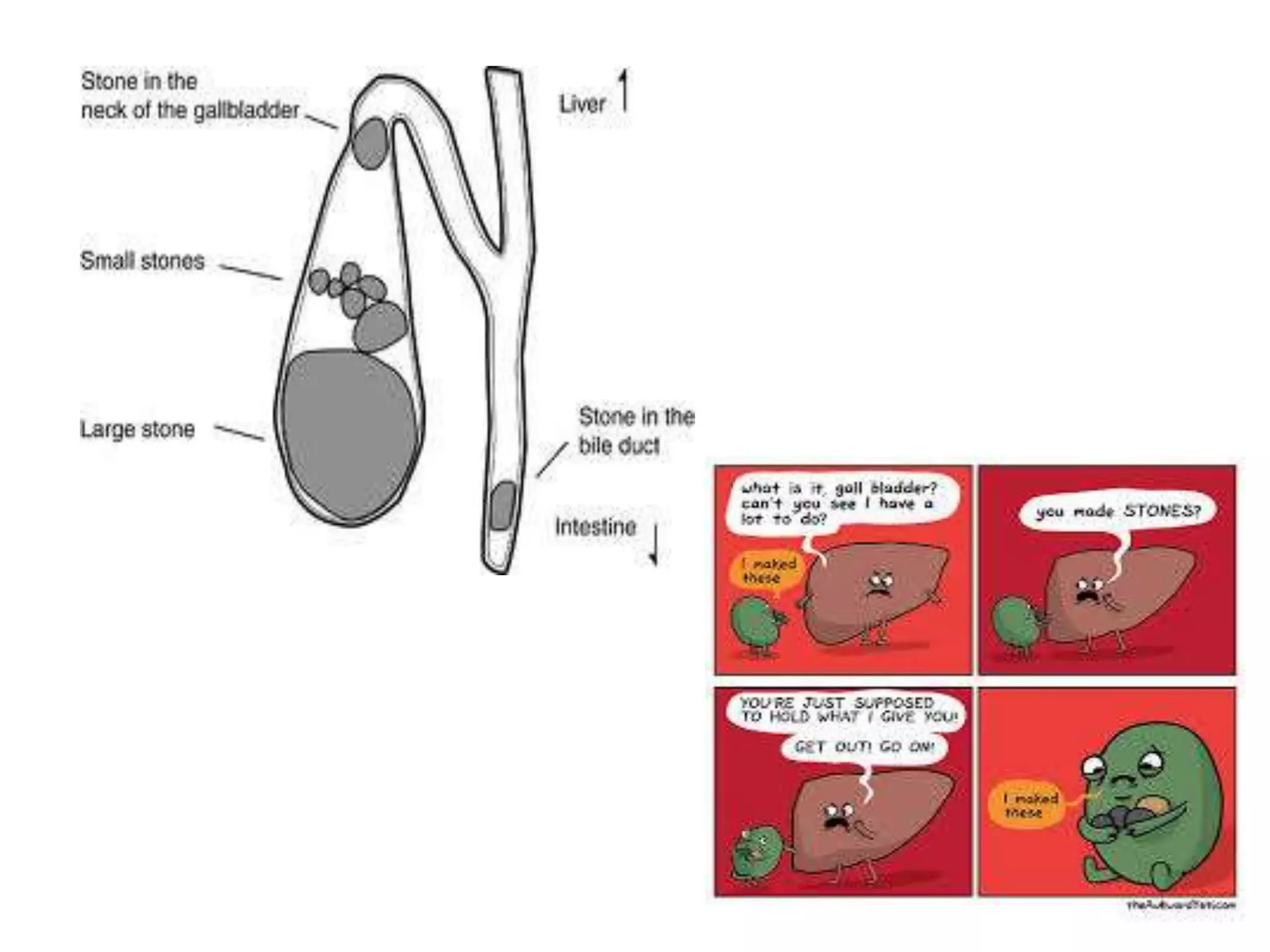
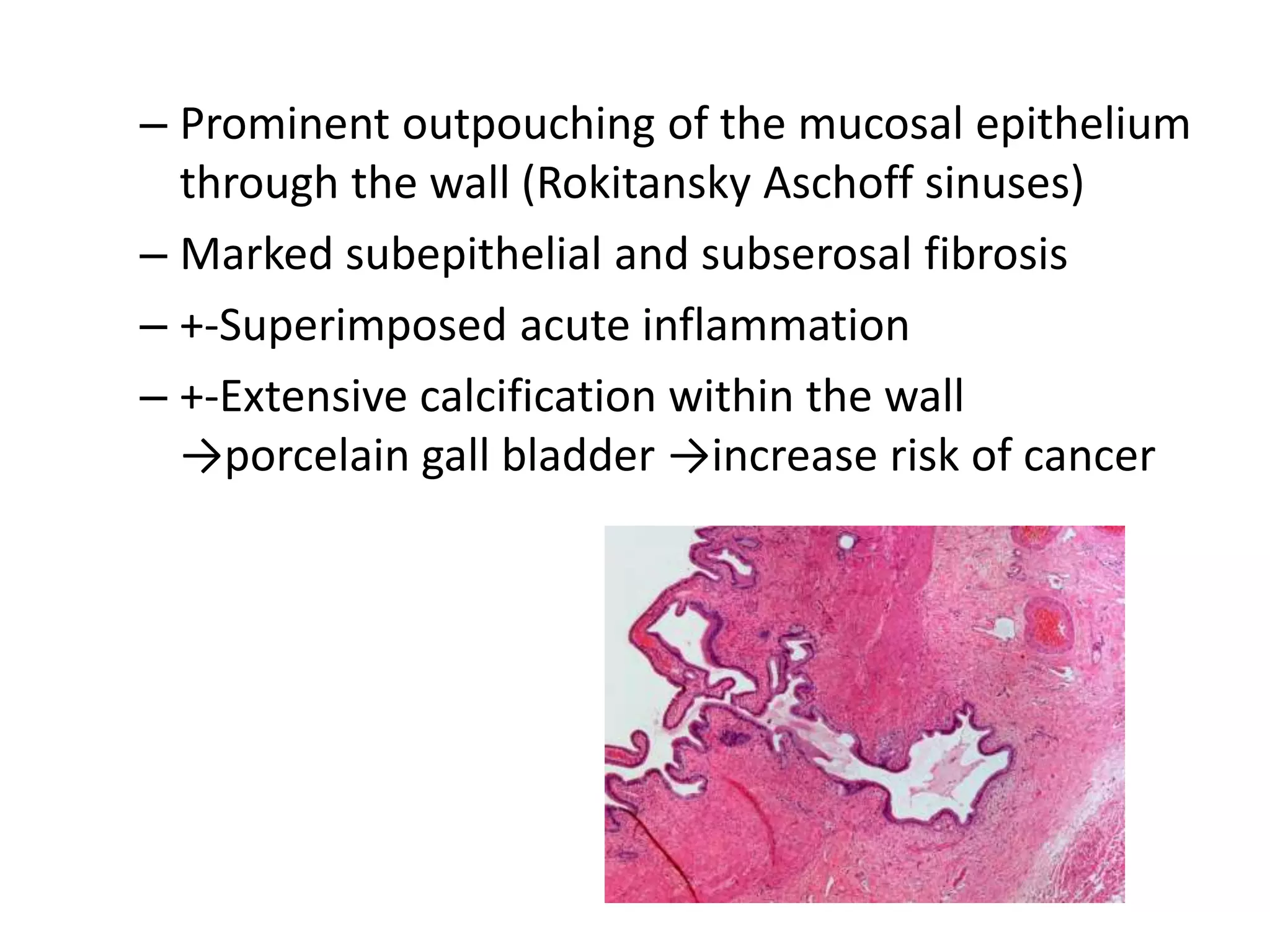
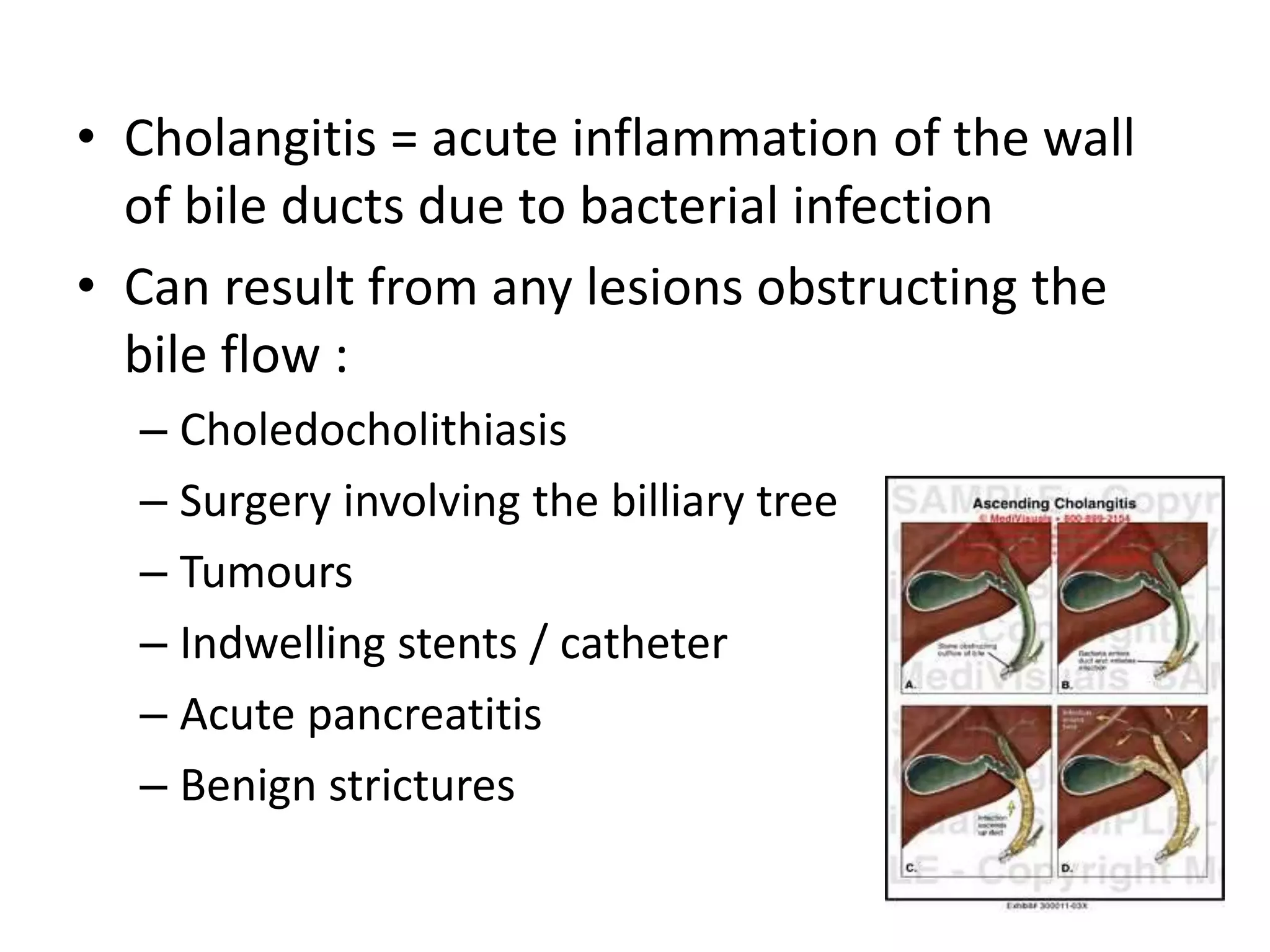
The document discusses various disorders of the gallbladder and bile ducts. It describes that over 95% of biliary tract diseases are due to cholelithiasis (gallstones), which can be either cholesterol stones or pigment stones. Cholecystitis, an inflammation of the gallbladder, can be acute or chronic and is usually caused by gallstones blocking the cystic duct. Other complications of gallbladder disorders include cholangitis, an inflammation of the bile ducts, and secondary biliary cirrhosis from long-term bile duct obstruction.