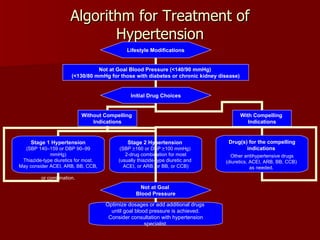
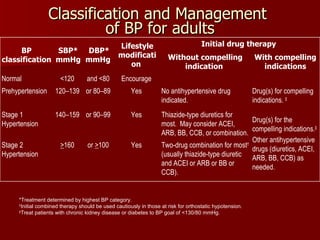
This document summarizes hypertension physiology, pathophysiology, and clinical management. It discusses the pathogenesis of primary hypertension including genetic and lifestyle factors. It also describes pathological changes in blood vessels and target organs. Symptoms, diagnosis, cardiovascular risk assessment, treatment goals, lifestyle modifications, and drug therapies are summarized. Treatment aims to reduce blood pressure below 140/90 mmHg or 130/80 mmHg for those with diabetes or kidney disease.