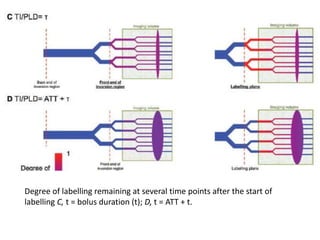
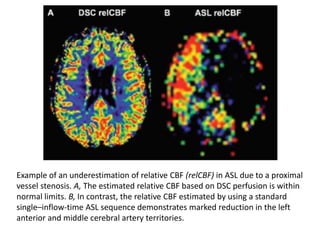
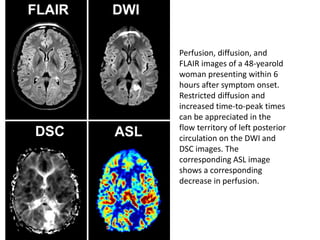
This document discusses arterial spin labeling (ASL), a noninvasive MRI technique used to measure cerebral blood flow. It describes the basic concepts and techniques of ASL, including pulsed ASL and pseudo-continuous ASL. Clinical applications include evaluating conditions like stroke, dementia, and tumors. The document outlines how ASL can detect perfusion deficits in acute ischemic stroke and discusses limitations such as lower signal-to-noise ratio compared to other perfusion techniques.









![Imaging in opaqe hemithorax [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/imaginginopaqehemithoraxautosaved-161030071708-thumbnail.jpg?width=640&height=640&fit=bounds)













































































