This document provides information on renal artery anatomy and Doppler ultrasound evaluation of the renal arteries. It describes:
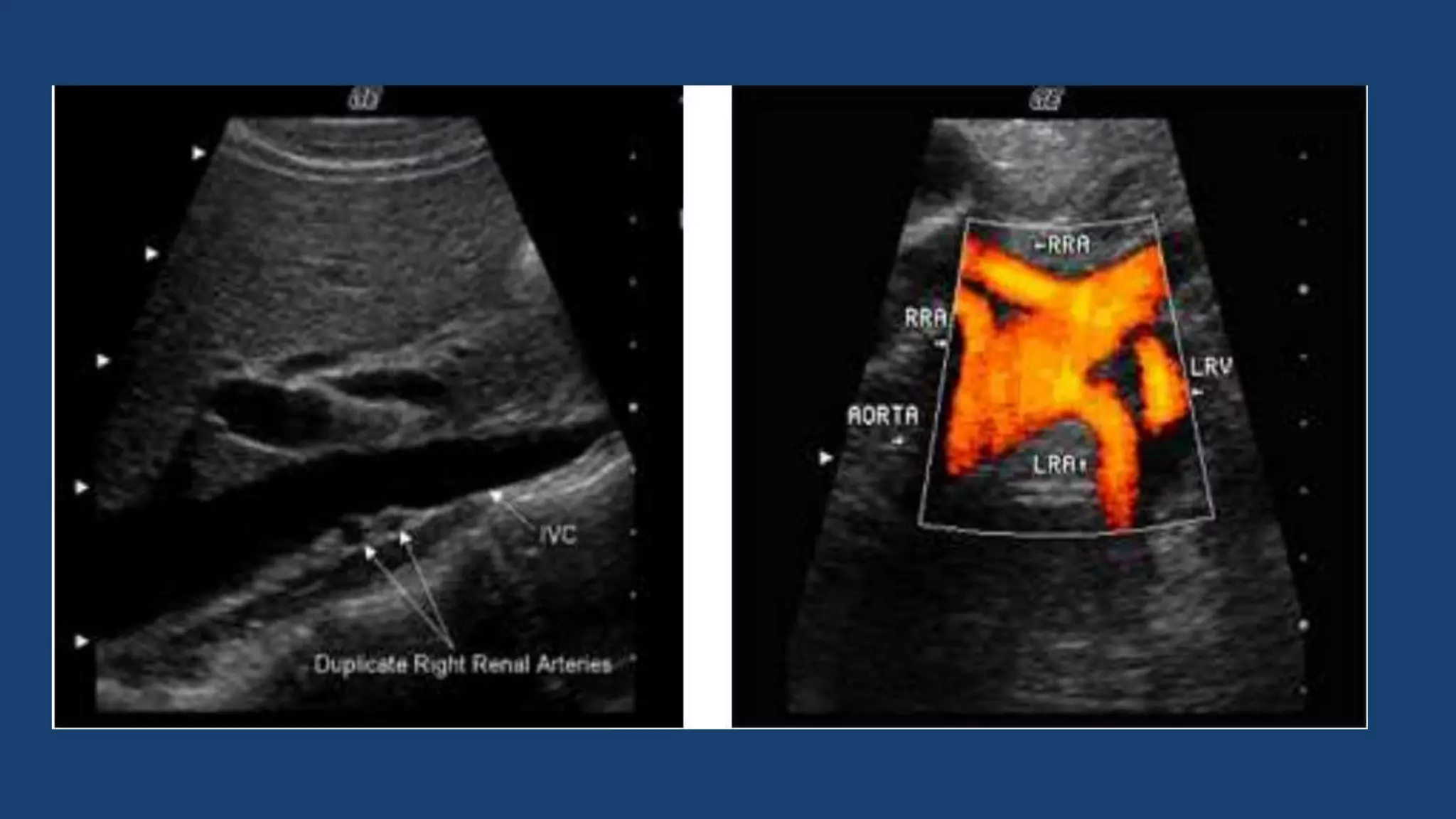
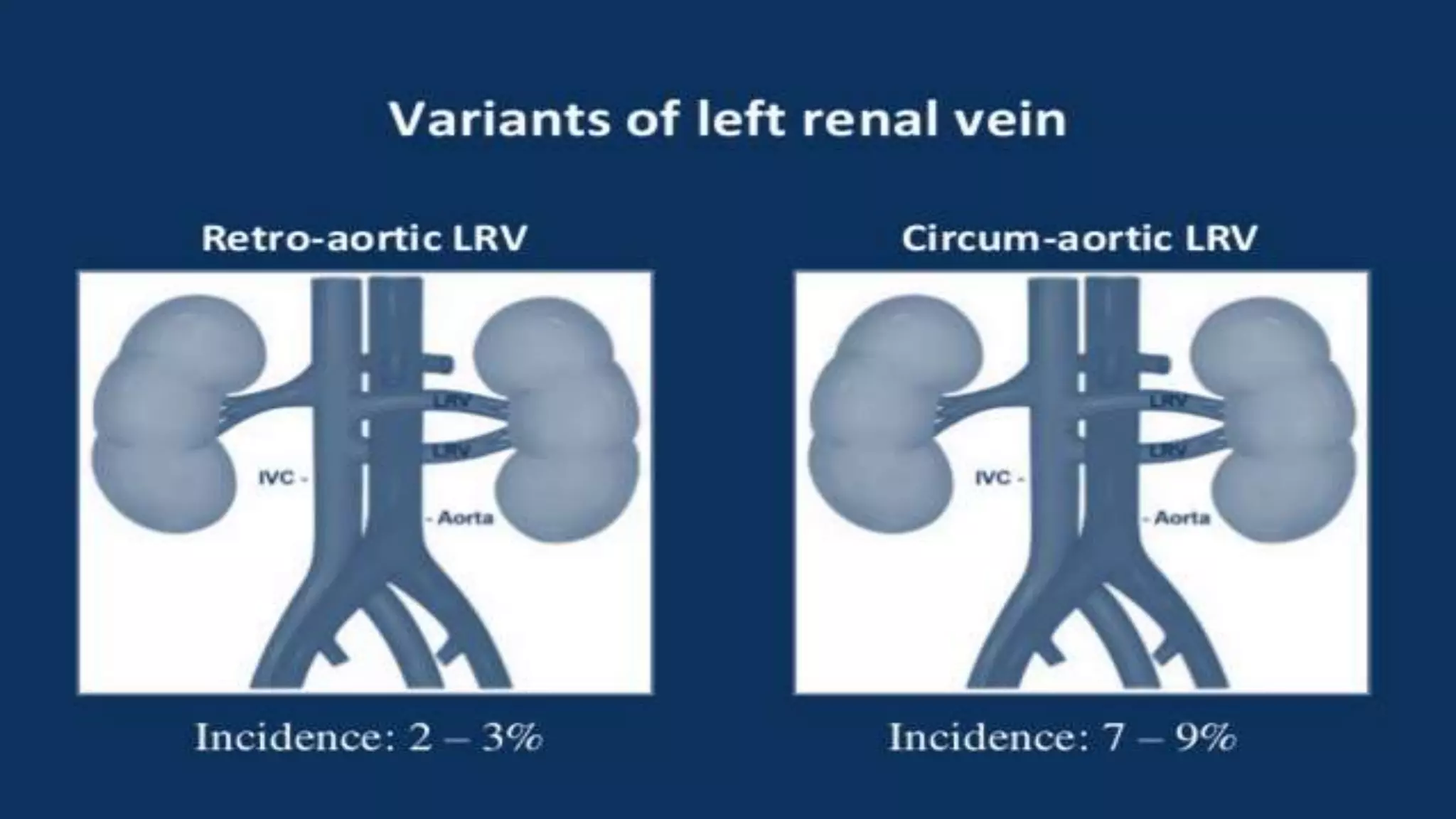
1. The typical origin and course of the right and left renal arteries. Approximately 30% of individuals have variant anatomy with more than one renal artery on each side.
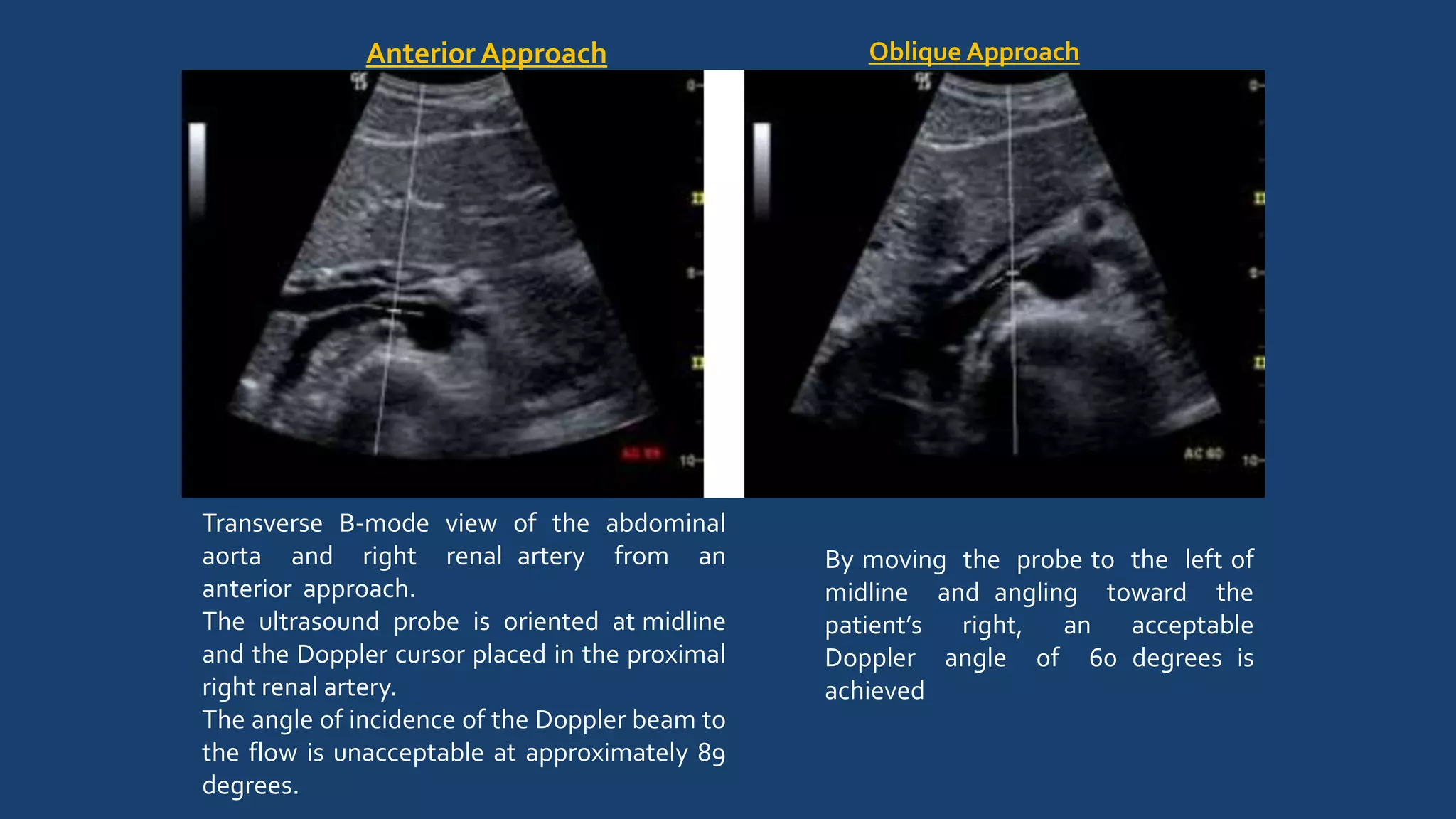
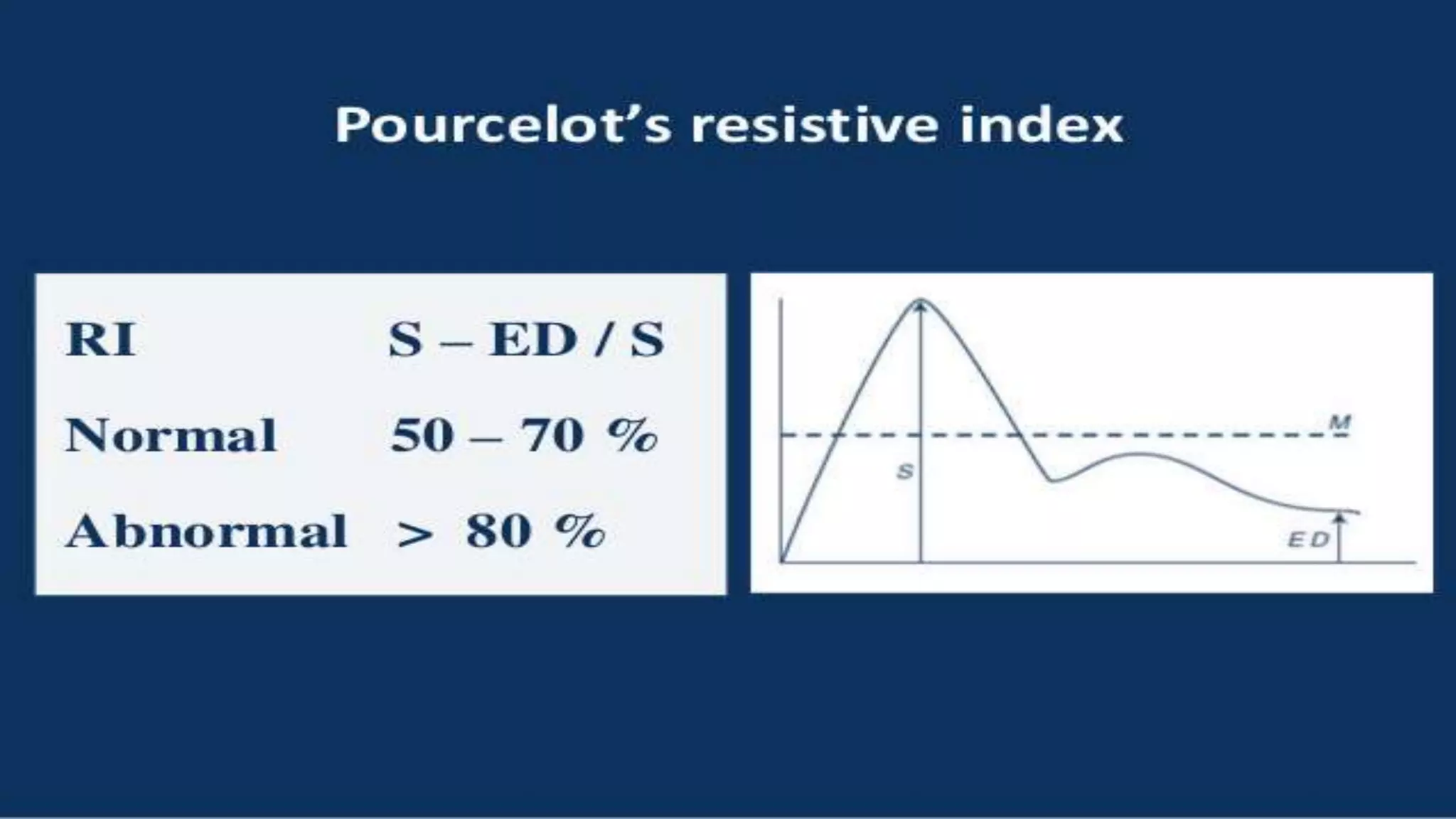
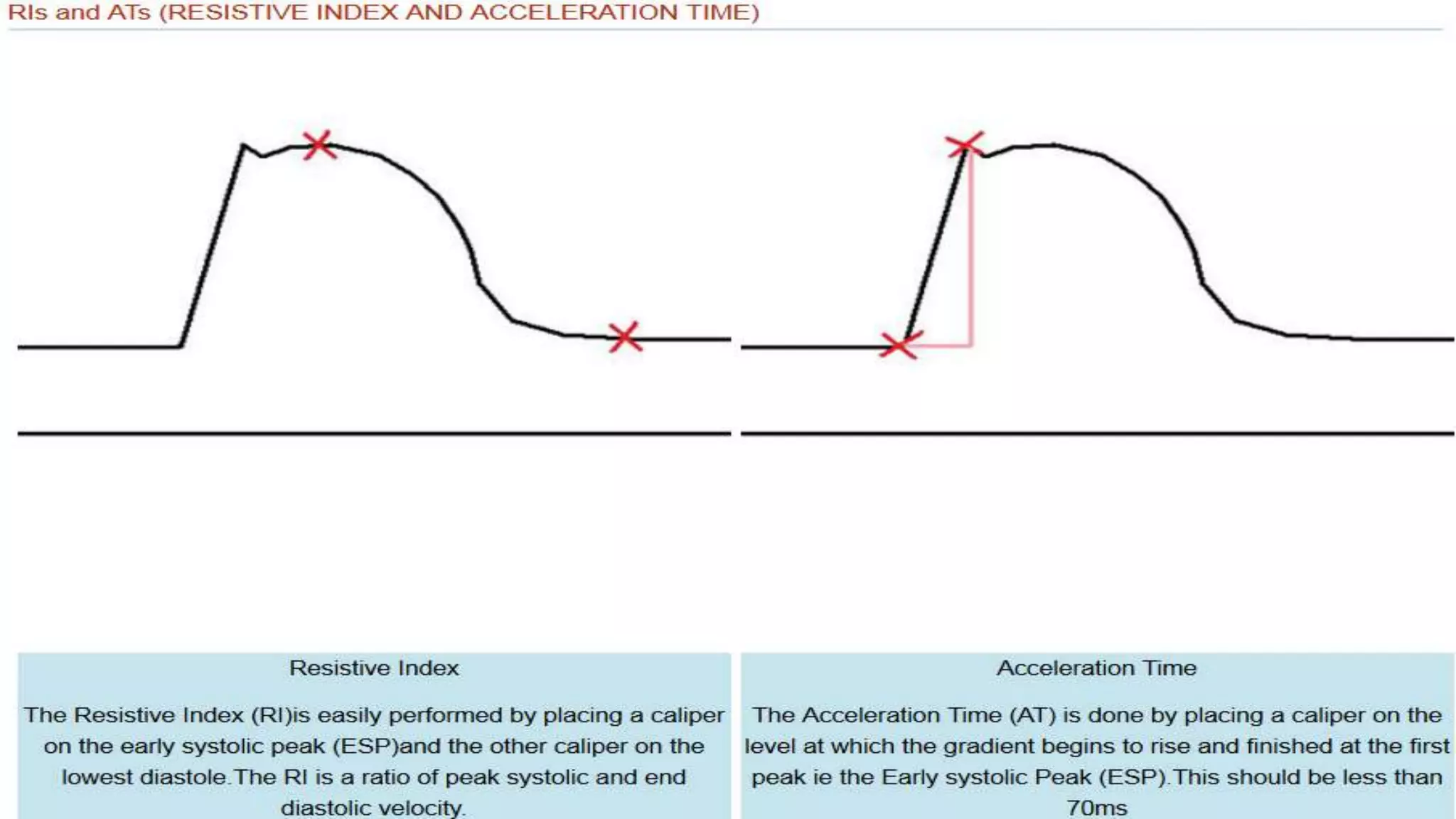
2. How Doppler ultrasound is used to image the renal arteries from different approaches and measure parameters like peak systolic velocity to evaluate for renal artery stenosis.
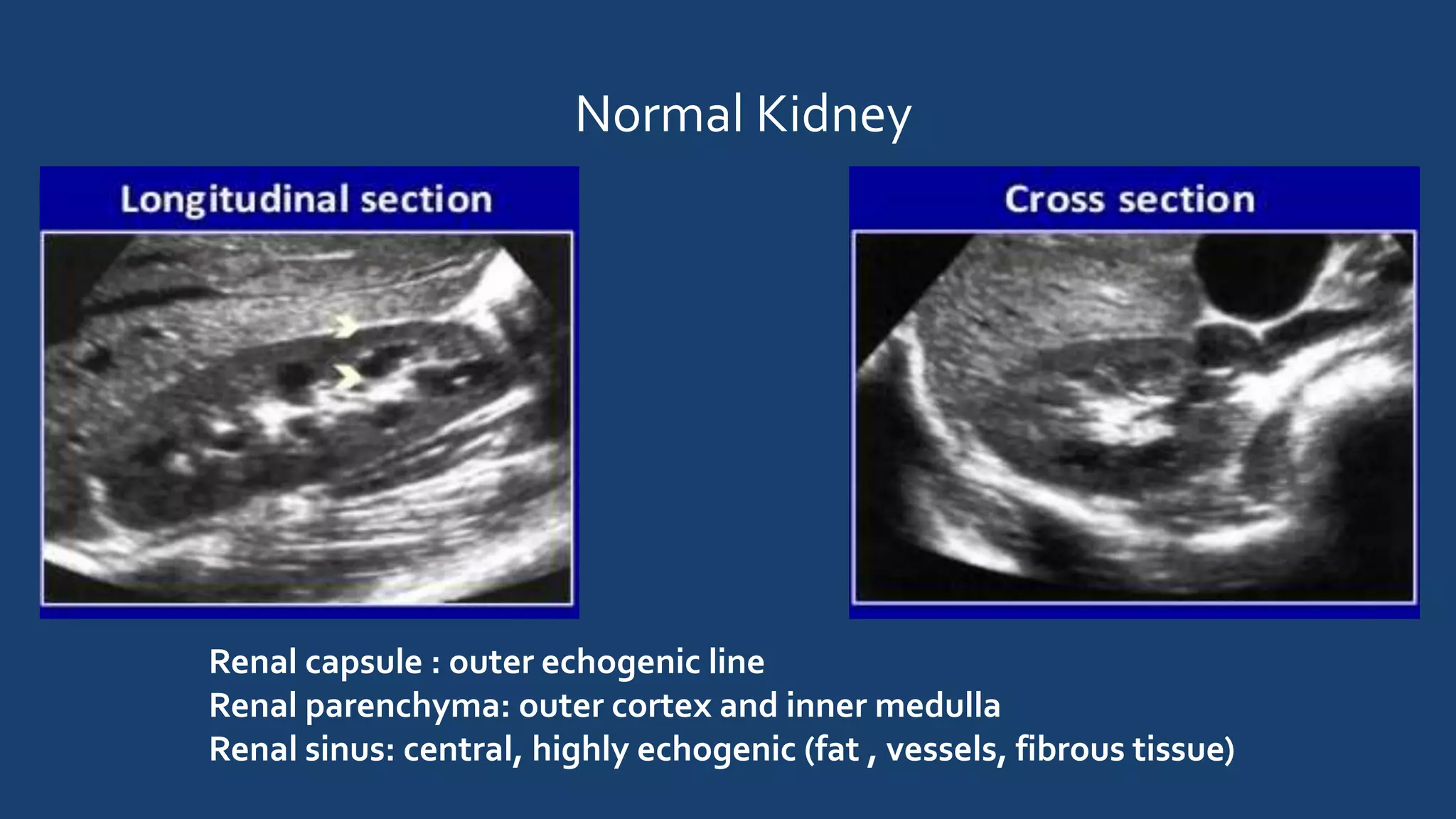
3. The normal Doppler waveforms expected in the main renal artery and intrarenal arteries, as well as normal values for measured parameters.
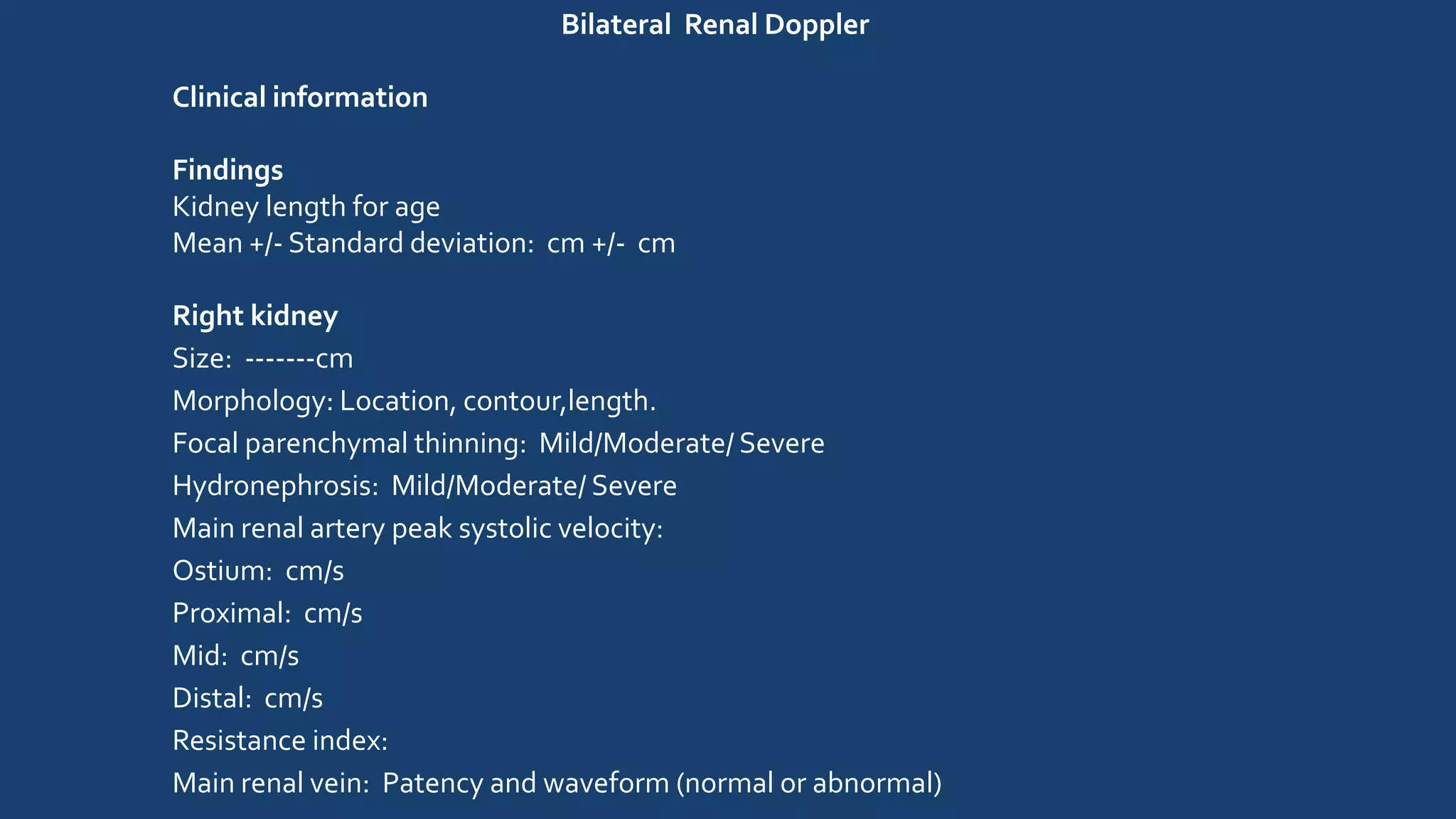
4. How a bilateral renal Doppler examination is performed, including evaluating each kidney, the renal arteries and veins, and measuring parameters to identify