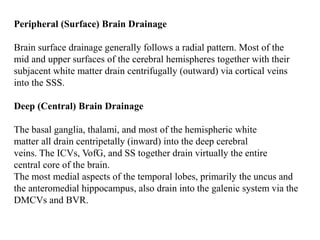
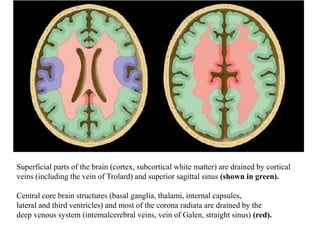
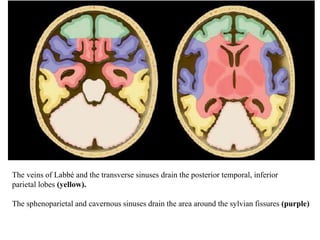
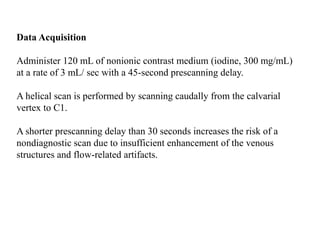
Superficial brain structures are drained by cortical veins and the superior sagittal sinus. Central brain structures drain into the deep venous system including the internal cerebral veins, vein of Galen, and straight sinus. The veins of Labbé and transverse sinuses drain the posterior temporal and inferior parietal lobes. MR venography and CT venography can assess the cerebral venous system, with each technique having advantages and disadvantages.
![Normal Venous Anatomy
The intracranial venous system has two major components,
Dural venous sinuses.
Cerebral veins.
Dural Venous Sinuses
Dural venous sinuses are subdivided into
Anteroinferior group [cavernous sinus (CS), superior and inferior
petrosal sinuses (SPSs, IPSs), clival venous plexus (CVP), and
sphenoparietal sinus (SphPS)]](https://image.slidesharecdn.com/ctvmrv-190917183810/85/CTV-and-MRV-2-320.jpg)
![Posterosuperior group [superior sagittal sinus (SSS), inferior sagittal
sinus (ISS), straight sinus (SS), sinus confluence (torcular herophili),
transverse sinuses (TSs), sigmoid sinuses, and jugular bulbs]
Cerebral Veins
The cerebral veins are subdivided into three groups:
(1) Superficial ("cortical" or "external") veins
I. Superior Cortical Veins [eight and twelve unnamed superficial veins,
vein of Trolard]
II. Middle Cortical Veins [superficial middle cerebral vein (SMCV)]
III. Inferior Cortical Veins [deep middle cerebral vein (DMCV), basal
vein of Rosenthal (BVR)]](https://image.slidesharecdn.com/ctvmrv-190917183810/85/CTV-and-MRV-3-320.jpg)
![(2) Deep cerebral ("internal") veins, and
I. Medullary veins
II. Subependymal veins,
III. Deep paramedian veins
(3) Brainstem/posterior fossa veins.
I. Superior ("galenic") group [ precentral cerebellar vein (PCV), the
superior vermian vein, and the anterior pontomesencephalic vein
(APMV)]
II. Anterior (petrosal) group [petrosal vein (PV)]
III. Posterior group [inferior vermian veins]](https://image.slidesharecdn.com/ctvmrv-190917183810/85/CTV-and-MRV-4-320.jpg)