Downloaded 84 times
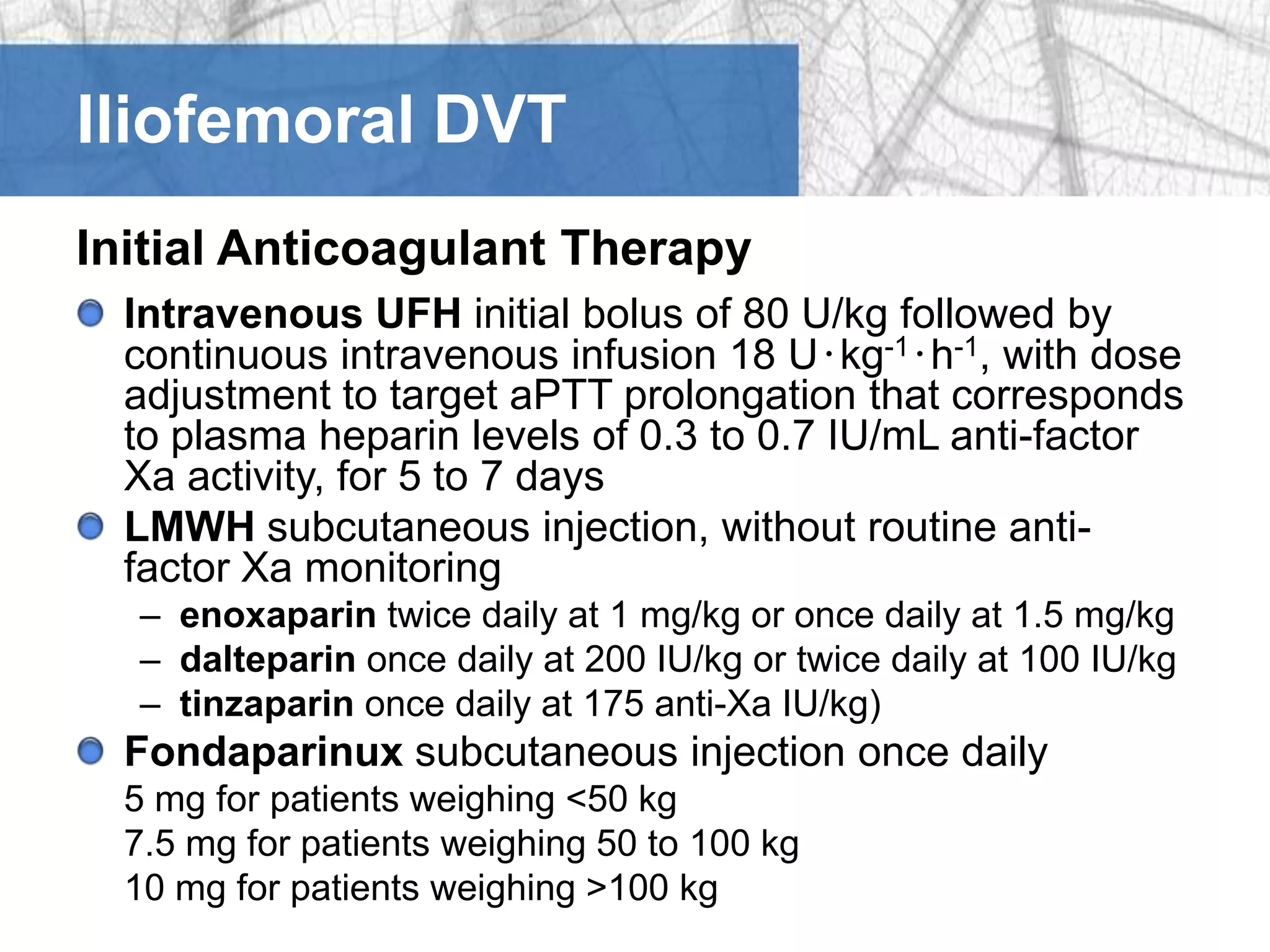
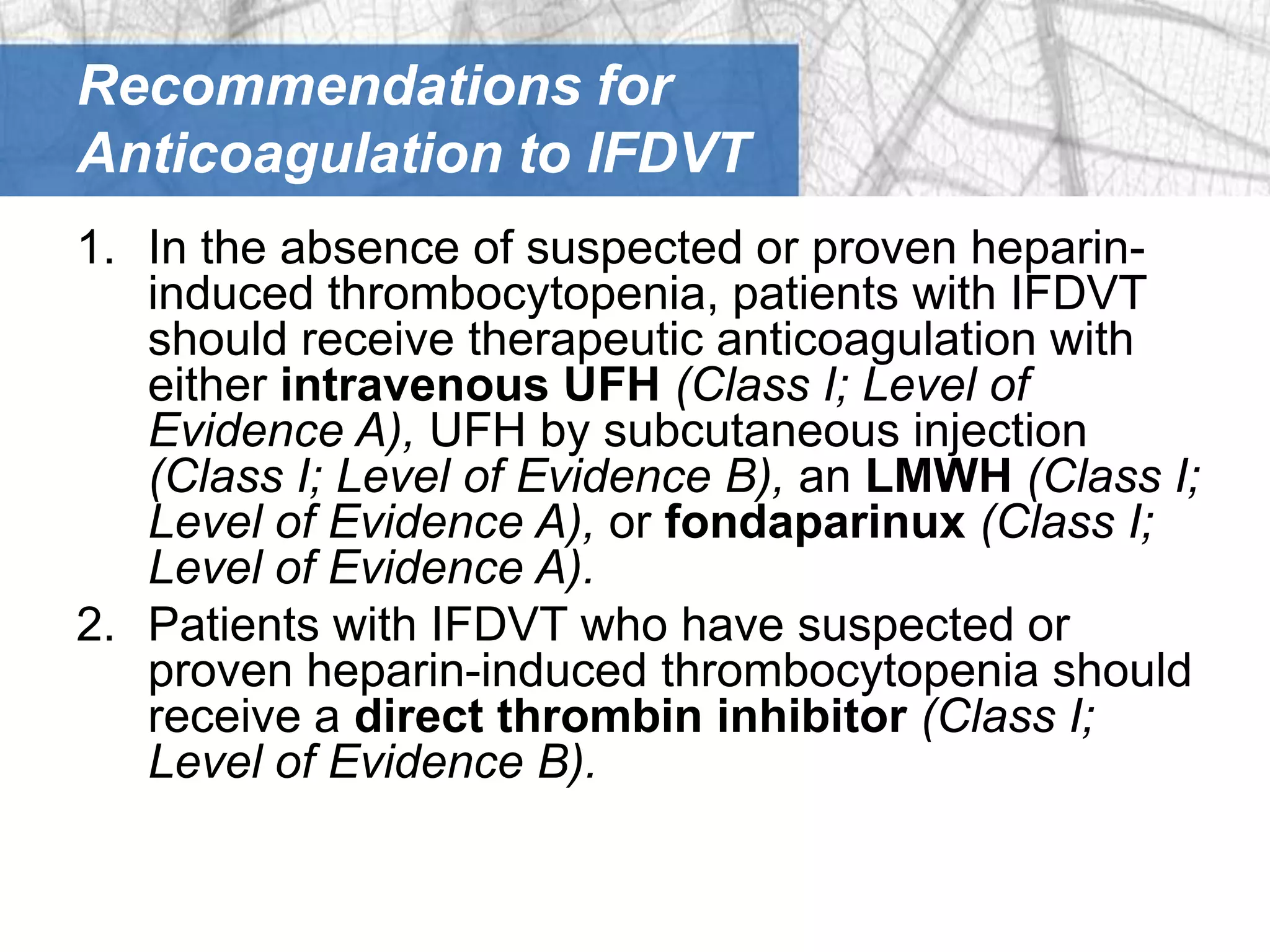
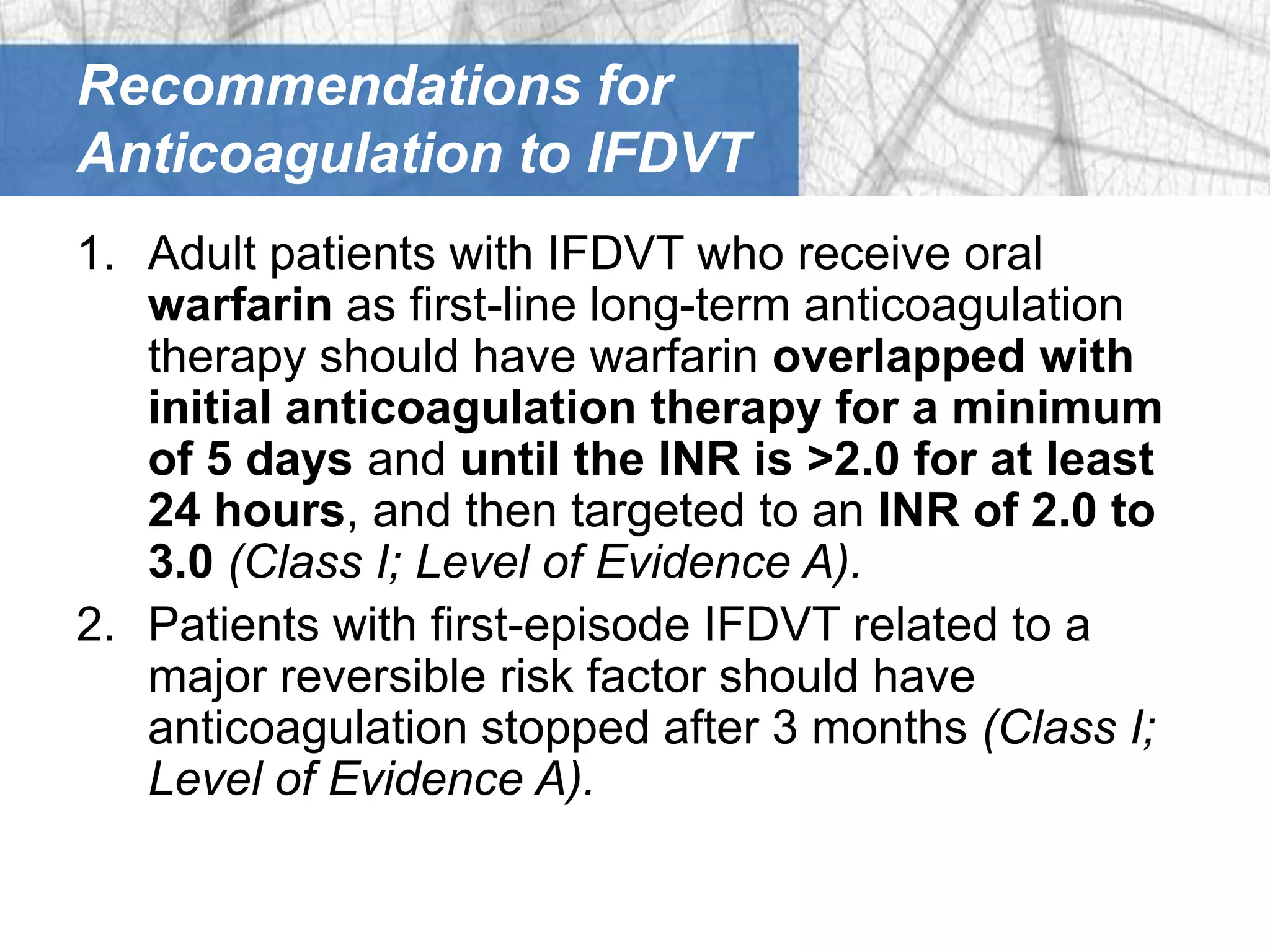
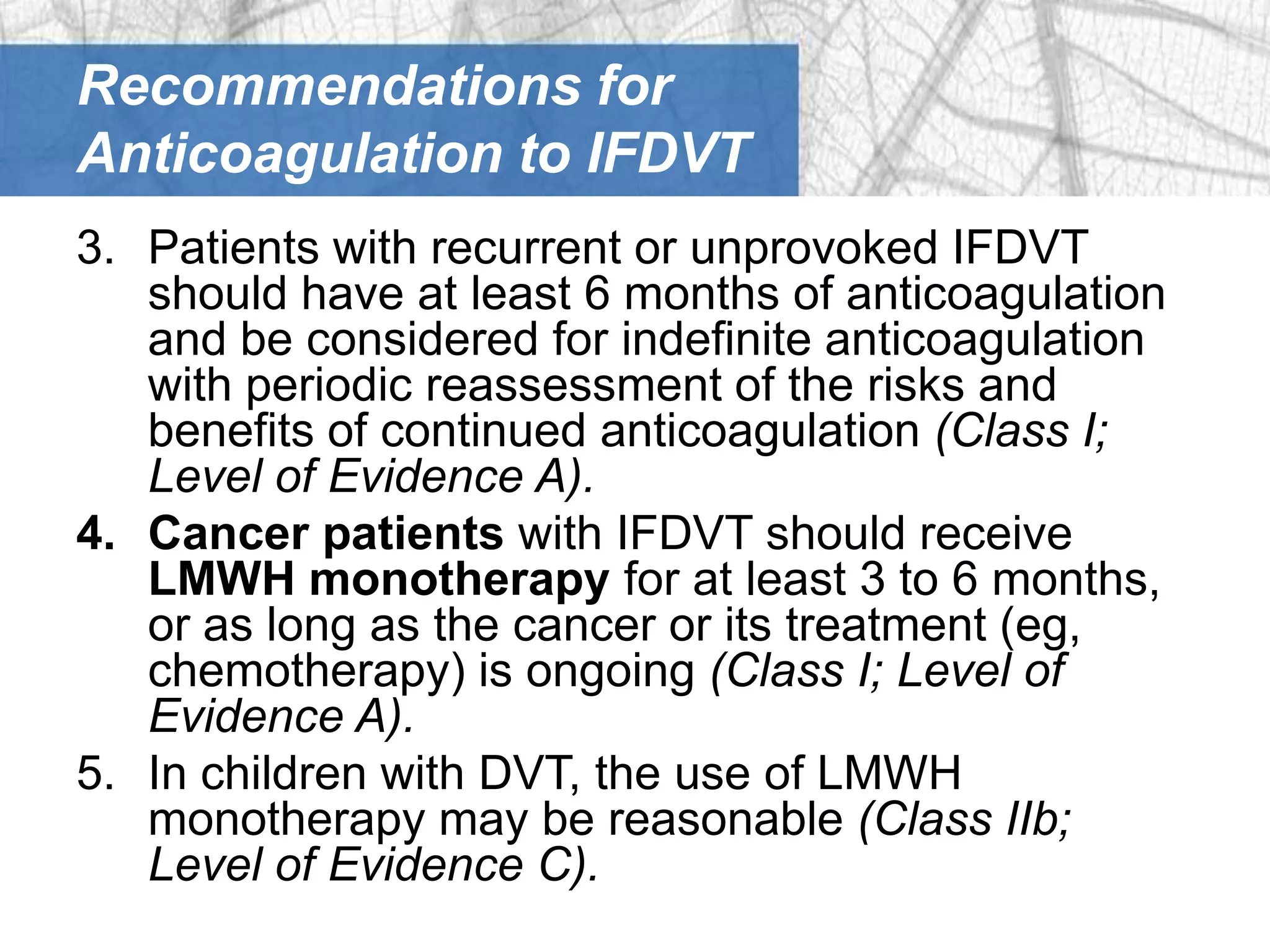
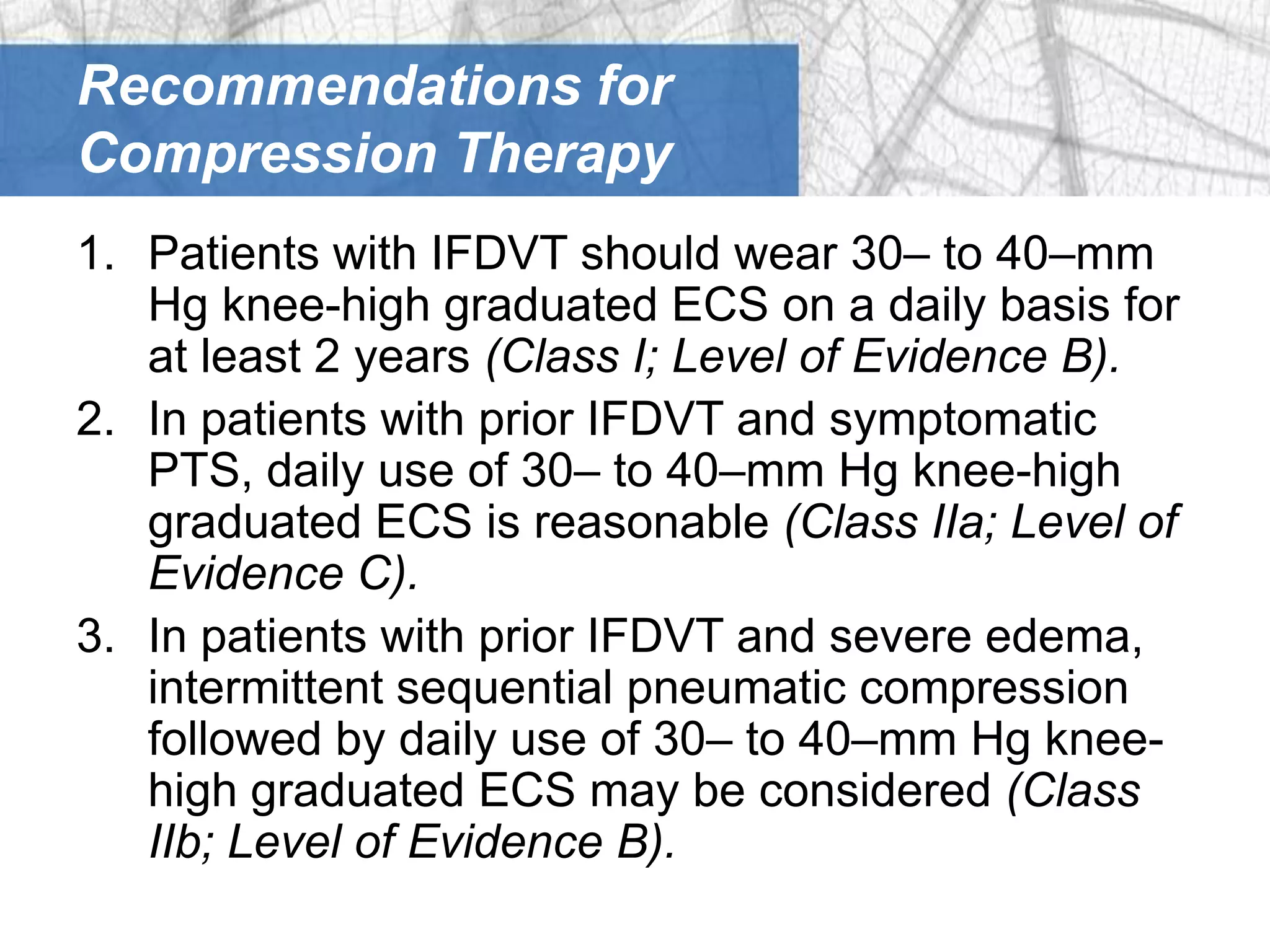
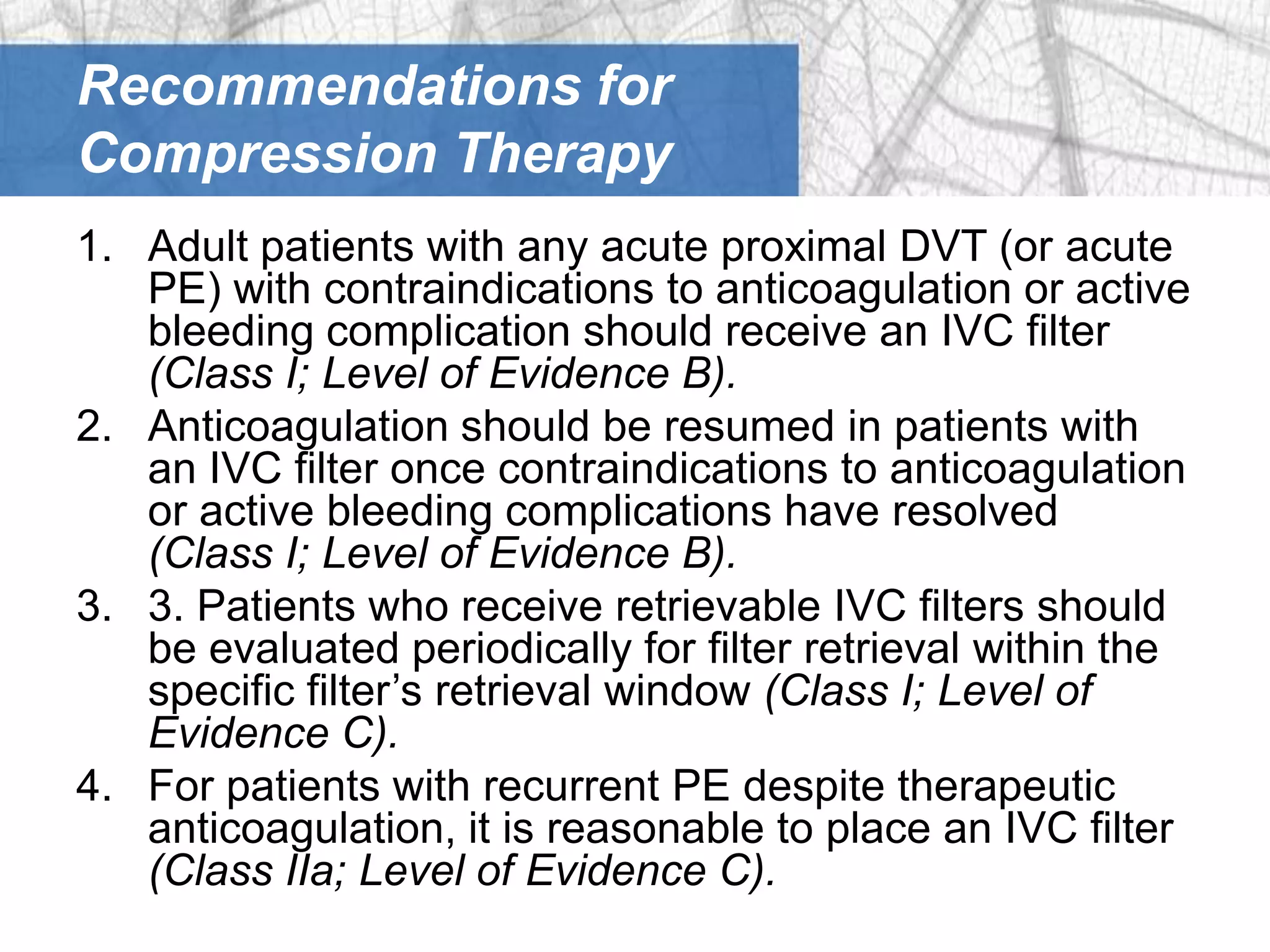
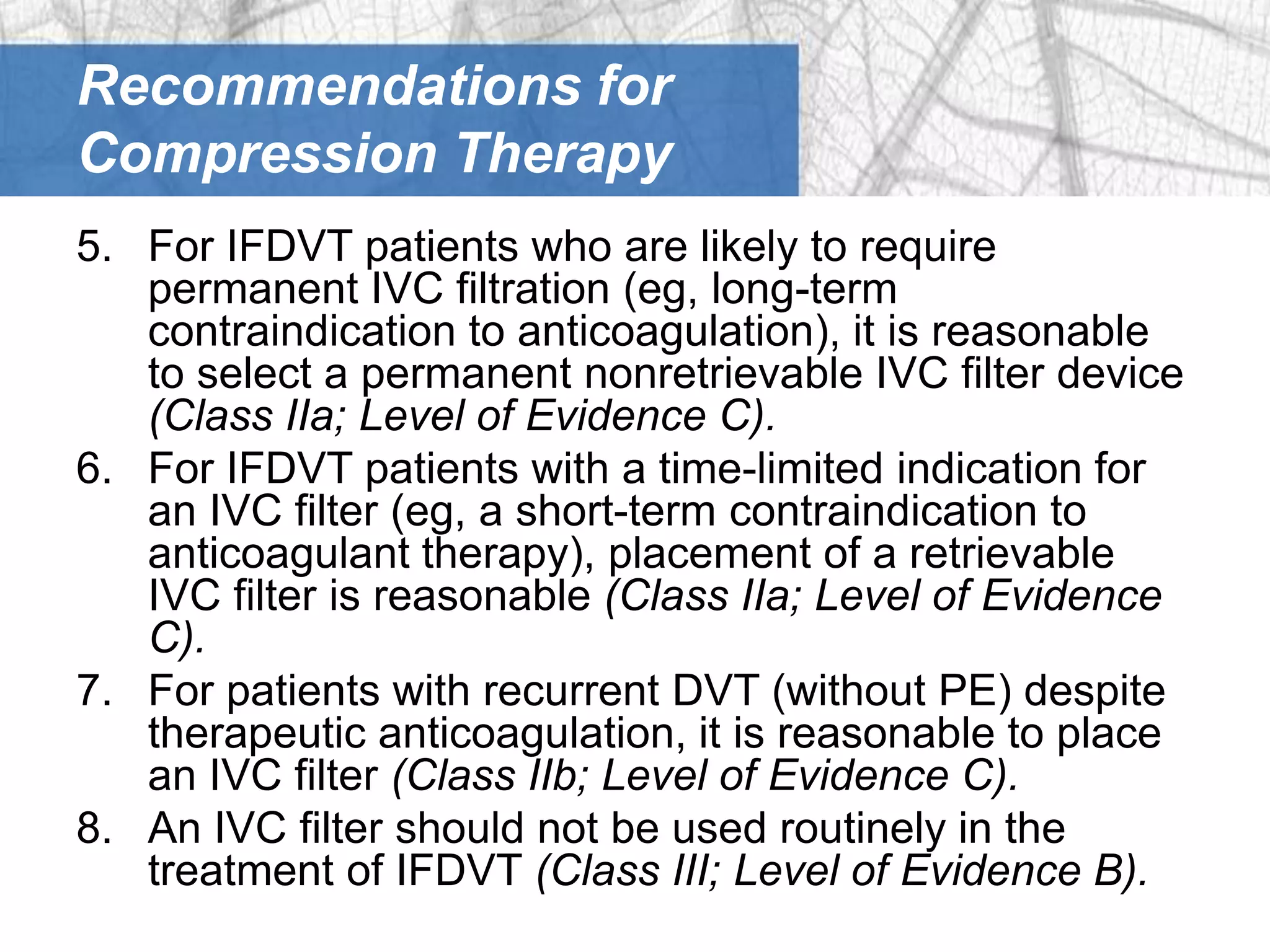
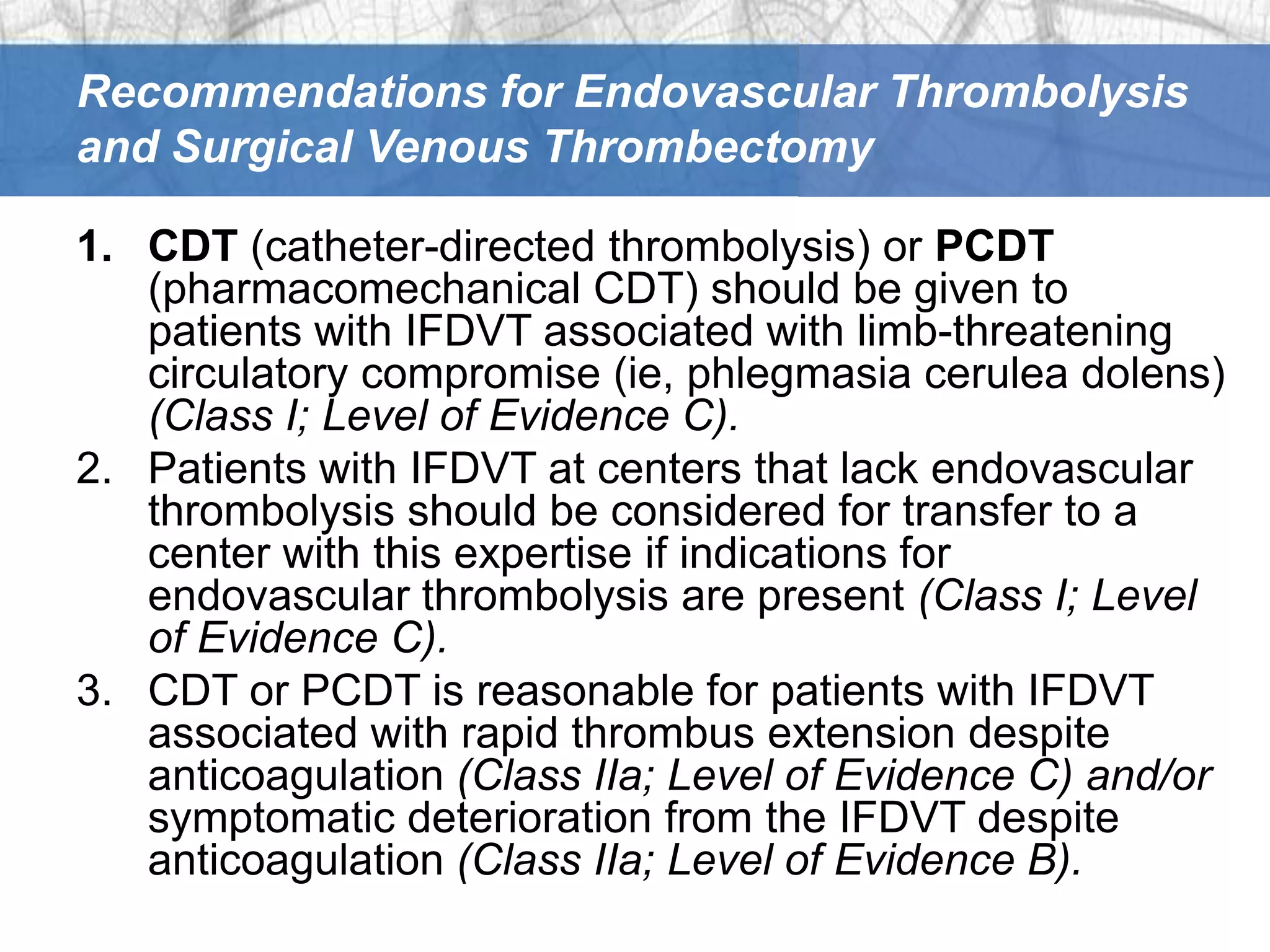
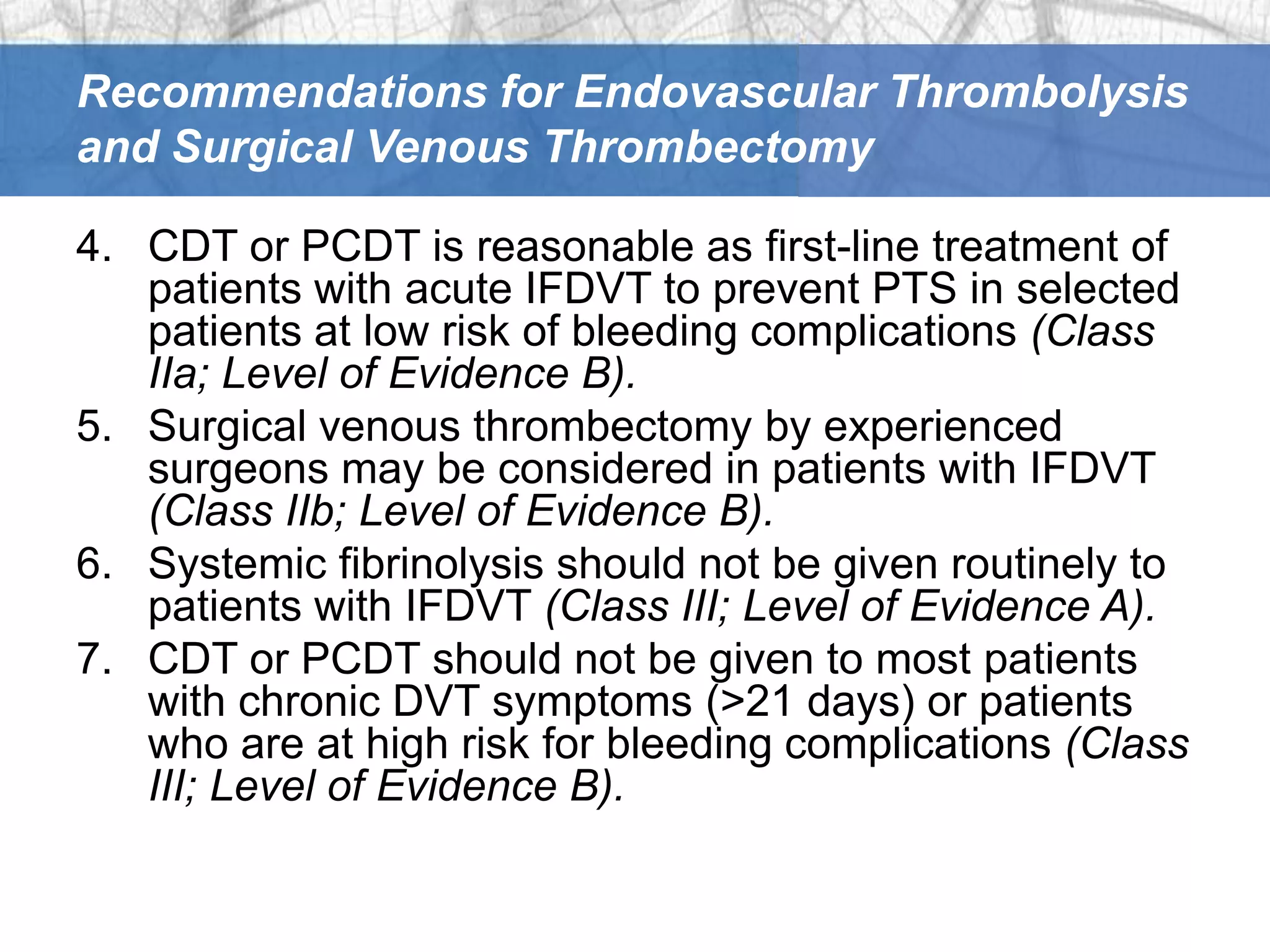
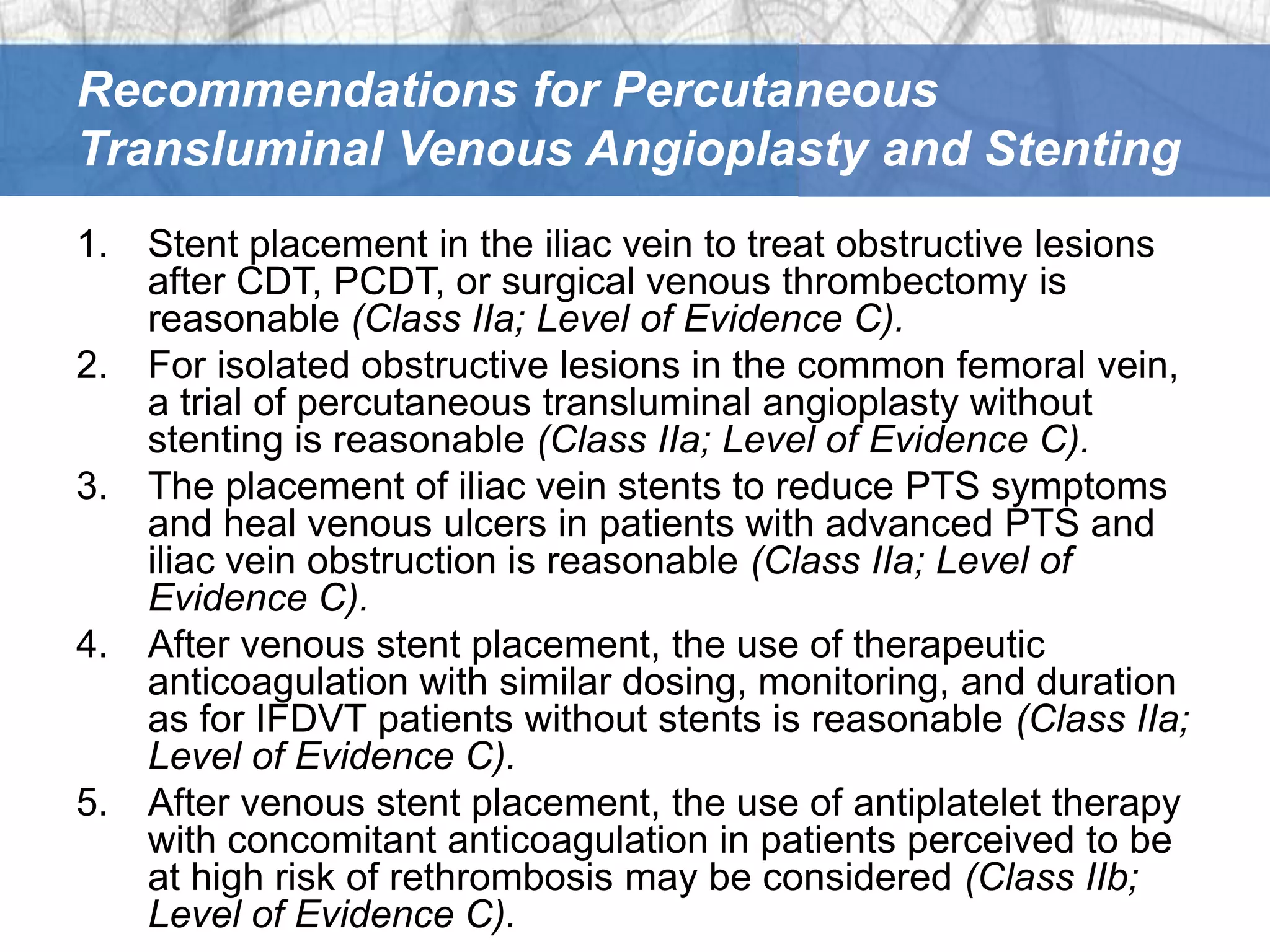

This document provides guidelines and recommendations for the management and treatment of iliofemoral deep vein thrombosis (IFDVT). It recommends initial anticoagulation therapy for IFDVT with unfractionated heparin, low molecular weight heparin, or fondaparinux. It provides guidance on duration of anticoagulation therapy based on risk factors. It also makes recommendations regarding compression therapy, inferior vena cava filters, endovascular thrombolysis, surgical thrombectomy, and percutaneous angioplasty/stenting.






































![PR CAMPAIGN 2011 [FRANCE]](https://cdn.slidesharecdn.com/ss_thumbnails/pipcarticleforafarfrenchfinal-130220044324-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































































