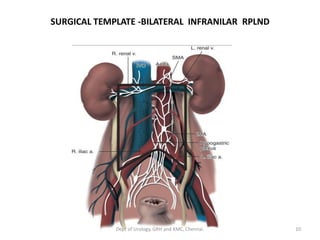
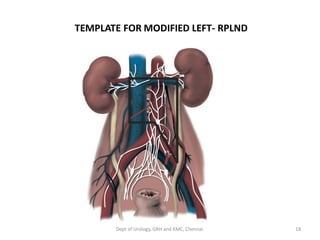
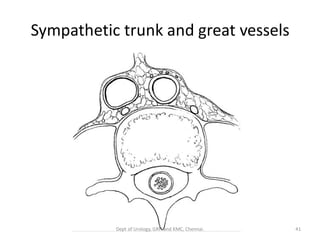
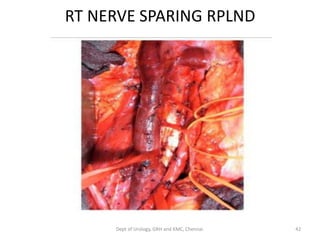
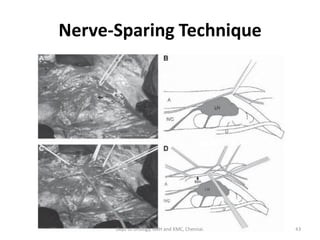
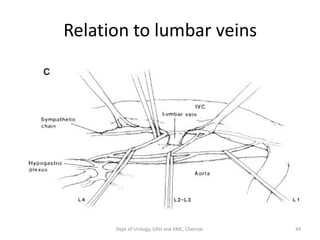
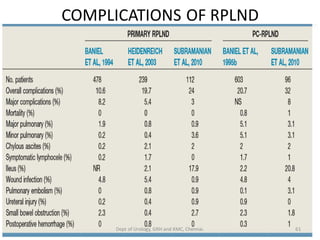
This document discusses retroperitoneal lymph node dissection (RPLND) and its complications. It provides a history of RPLND, describes the lymphatic drainage patterns of the testis and rationale for RPLND. It outlines the evolution of surgical templates for RPLND including modifications to reduce complications like loss of antegrade ejaculation. The document discusses indications for primary, post-chemotherapy and salvage RPLND. It provides details of surgical techniques including approaches, lymphadenectomy procedures and nerve-sparing techniques.