Downloaded 1,570 times




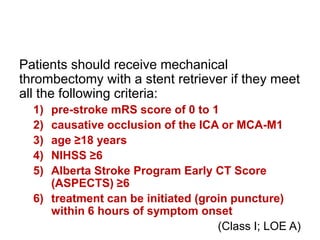




The 2018 acute ischemic stroke guidelines emphasize rapid prehospital notification and patient transport to appropriate hospitals capable of administering IV alteplase. Key recommendations include achieving door-to-needle times within 60 minutes, ensuring brain imaging within 20 minutes of ED arrival, and maintaining blood pressure thresholds for IV alteplase administration. Additionally, the guidelines endorse mechanical thrombectomy for eligible patients and detail criteria for various treatments based on individual patient circumstances.


![Management of acute ischemic stroke including tia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofacuteischemicstrokeincludingtiaautosaved-180808183403-thumbnail.jpg?width=640&height=640&fit=bounds)
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















