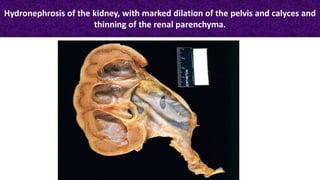
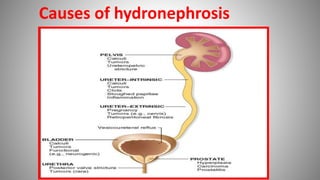
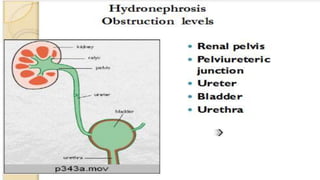
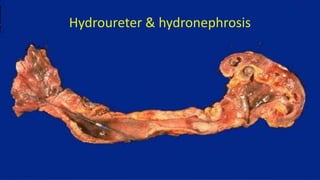
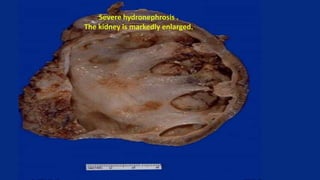
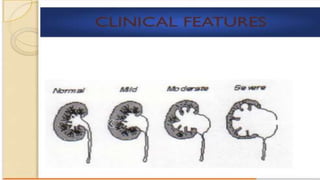
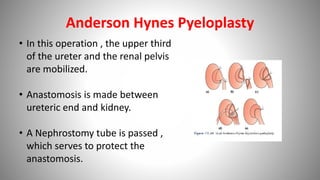
Hydronephrosis is the dilatation of the renal pelvis and calyces caused by obstruction of urine flow from the kidney. It can be caused by congenital abnormalities, such as ureteral atresia, or acquired issues like kidney stones. On imaging, the kidney appears enlarged with a distended pelvis and thinning of the renal parenchyma. Treatment depends on the severity and cause of obstruction, ranging from nephrostomy or pyeloplasty for mild hydronephrosis to nephrectomy if the kidney is non-functioning.