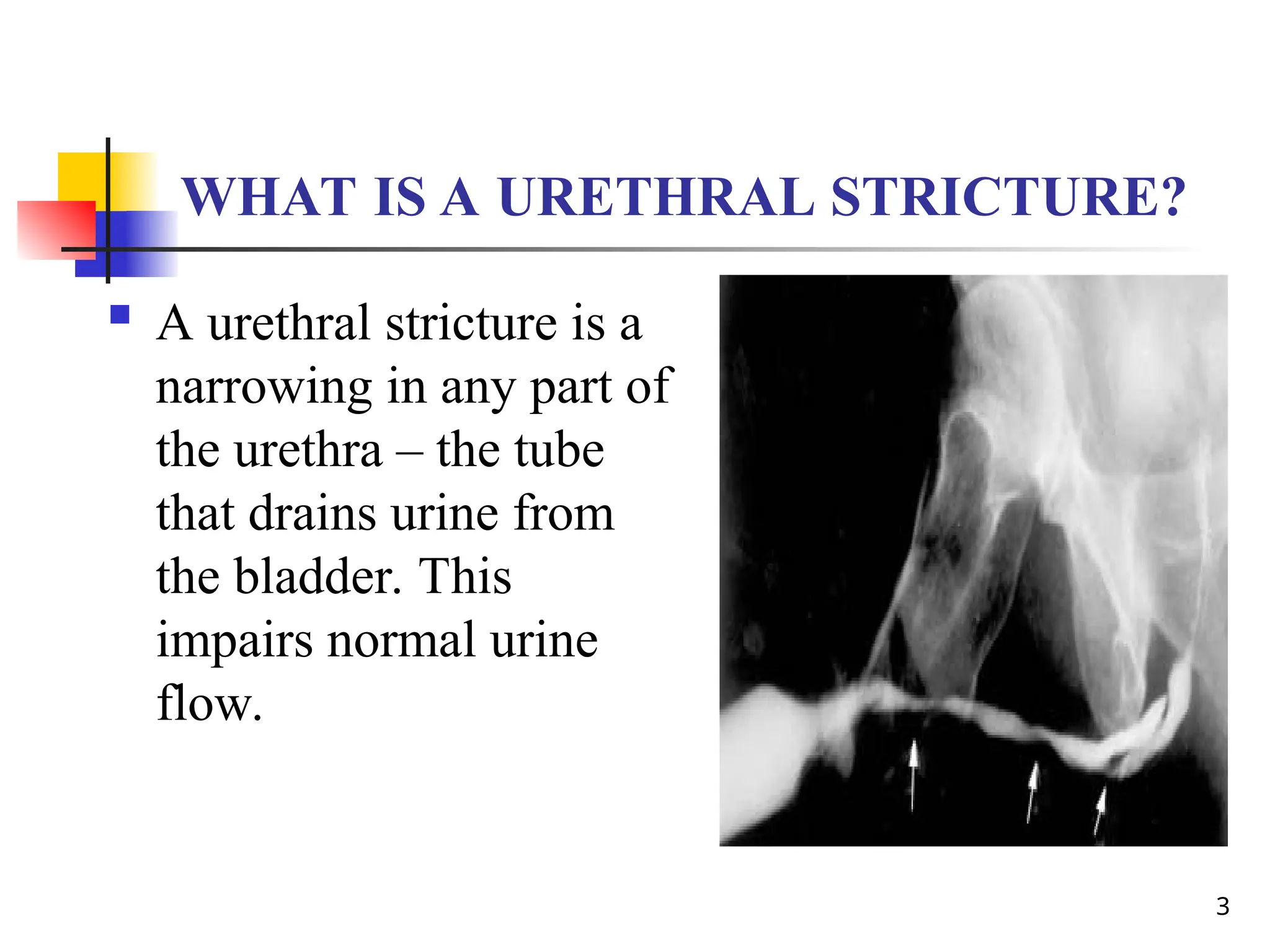
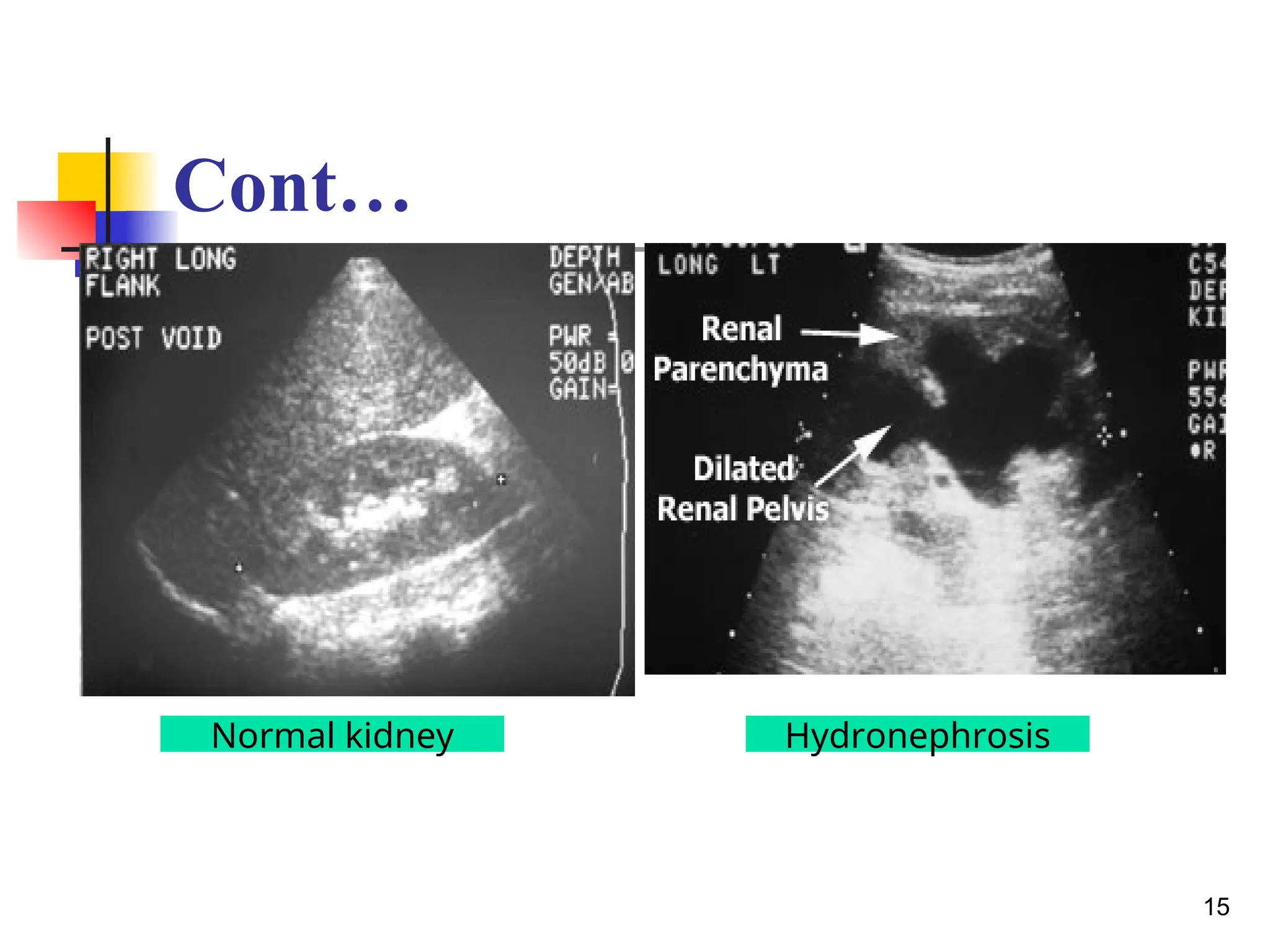
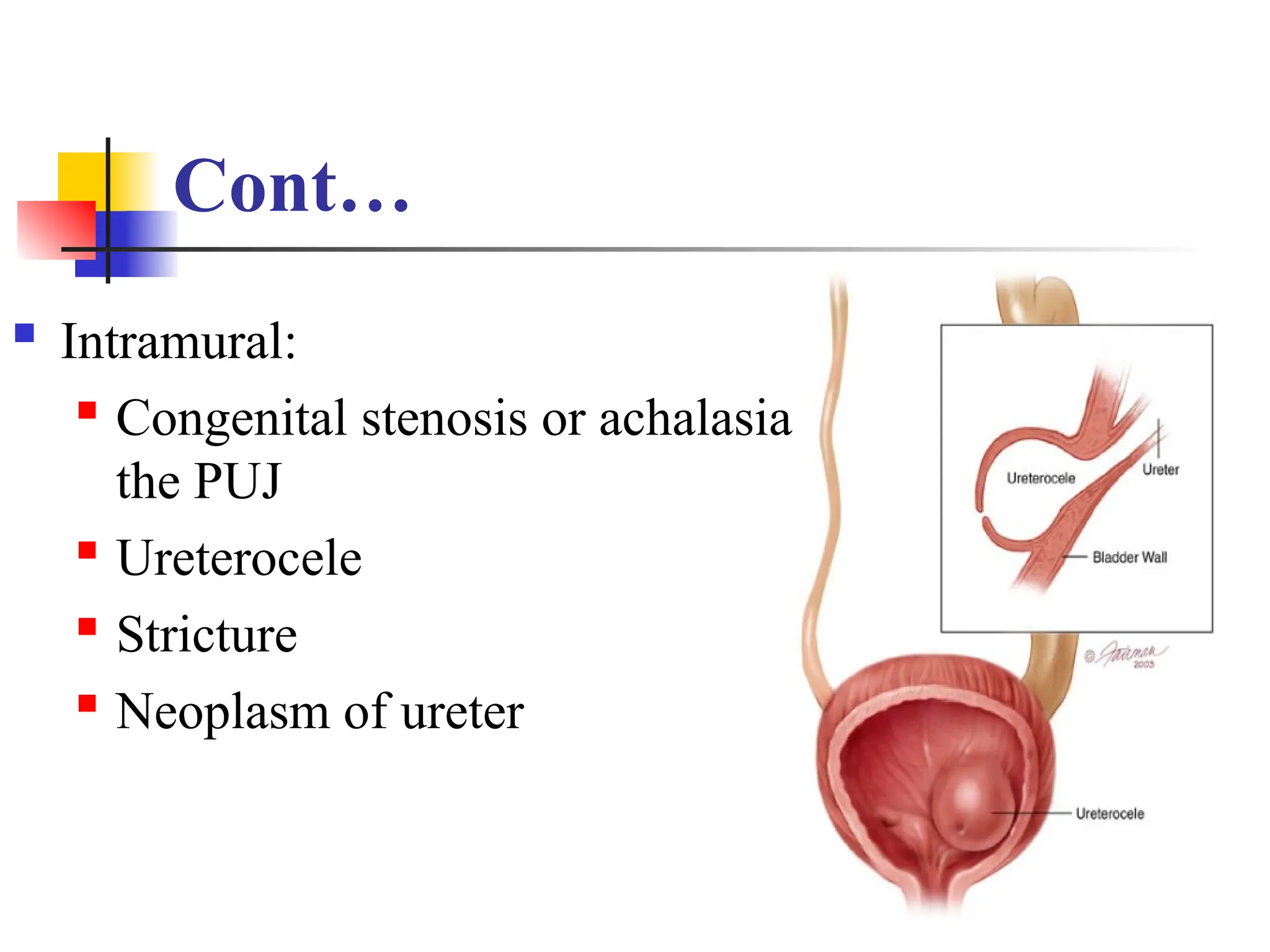
The document discusses urethral strictures and hydronephrosis, covering their causes, symptoms, diagnostics, and management. Urethral strictures result from narrowing of the urethra affecting urine flow, with various treatments including surgery and catheterization. Hydronephrosis is characterized by kidney dilation due to urine outflow obstruction, with causes ranging from tumors to congenital issues, and is also managed through surgical interventions.