Downloaded 404 times
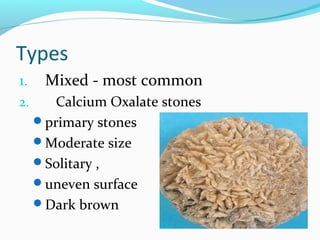



This document defines and describes different types of bladder stones. Primary stones develop in sterile urine, while secondary stones occur due to infection, outflow obstruction, or impaired bladder emptying. The most common type is mixed stones. Diagnosis involves urinalysis, ultrasound, and radiography. Treatment depends on the cause but may include lithotripsy, percutaneous litholapaxy, or catheter removal to break up the stones. Various modalities like lithotrites, lasers, and evacuators are used for fragmentation and removal of stones and stone fragments from the bladder.























































































