Downloaded 906 times
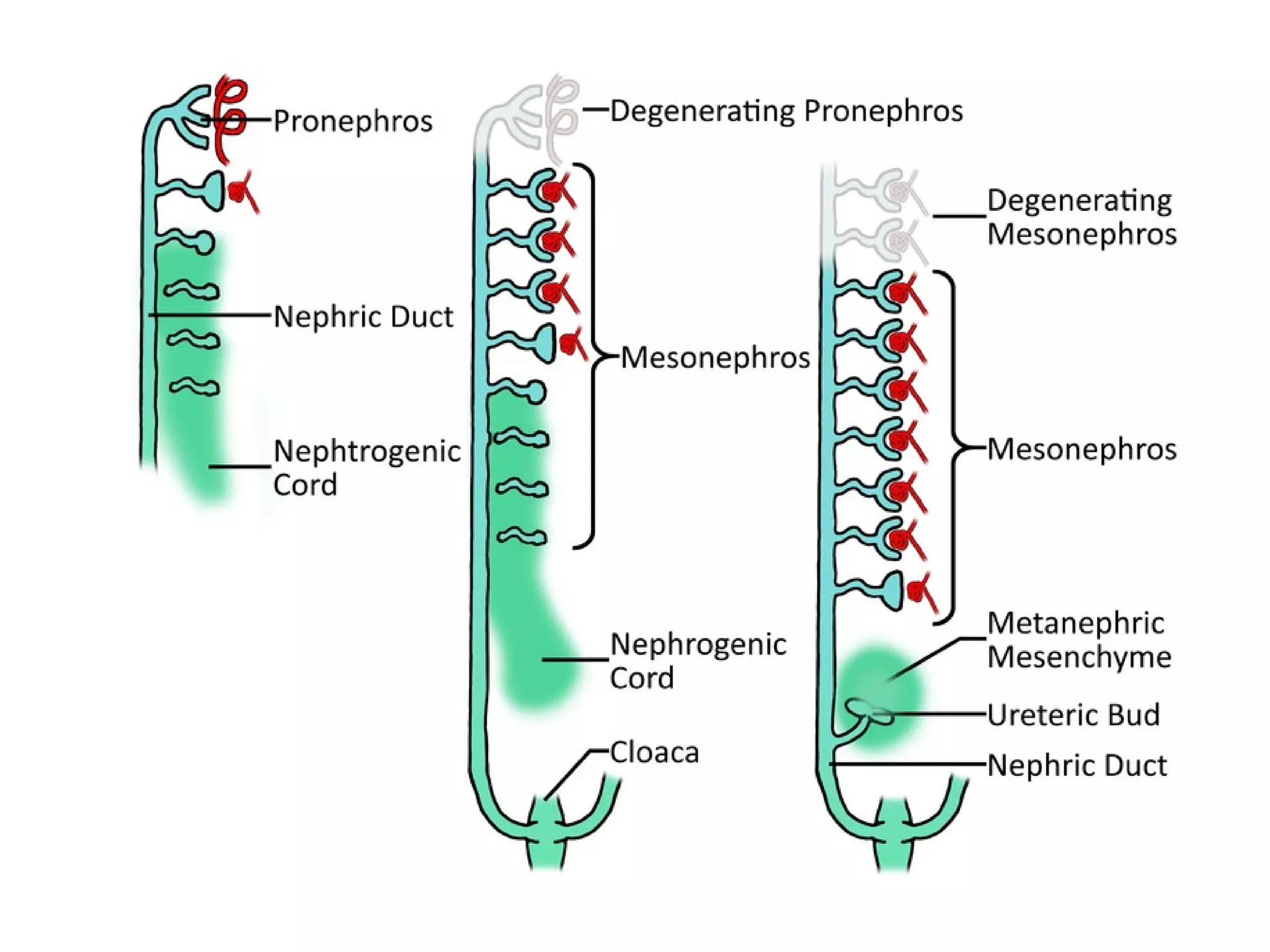
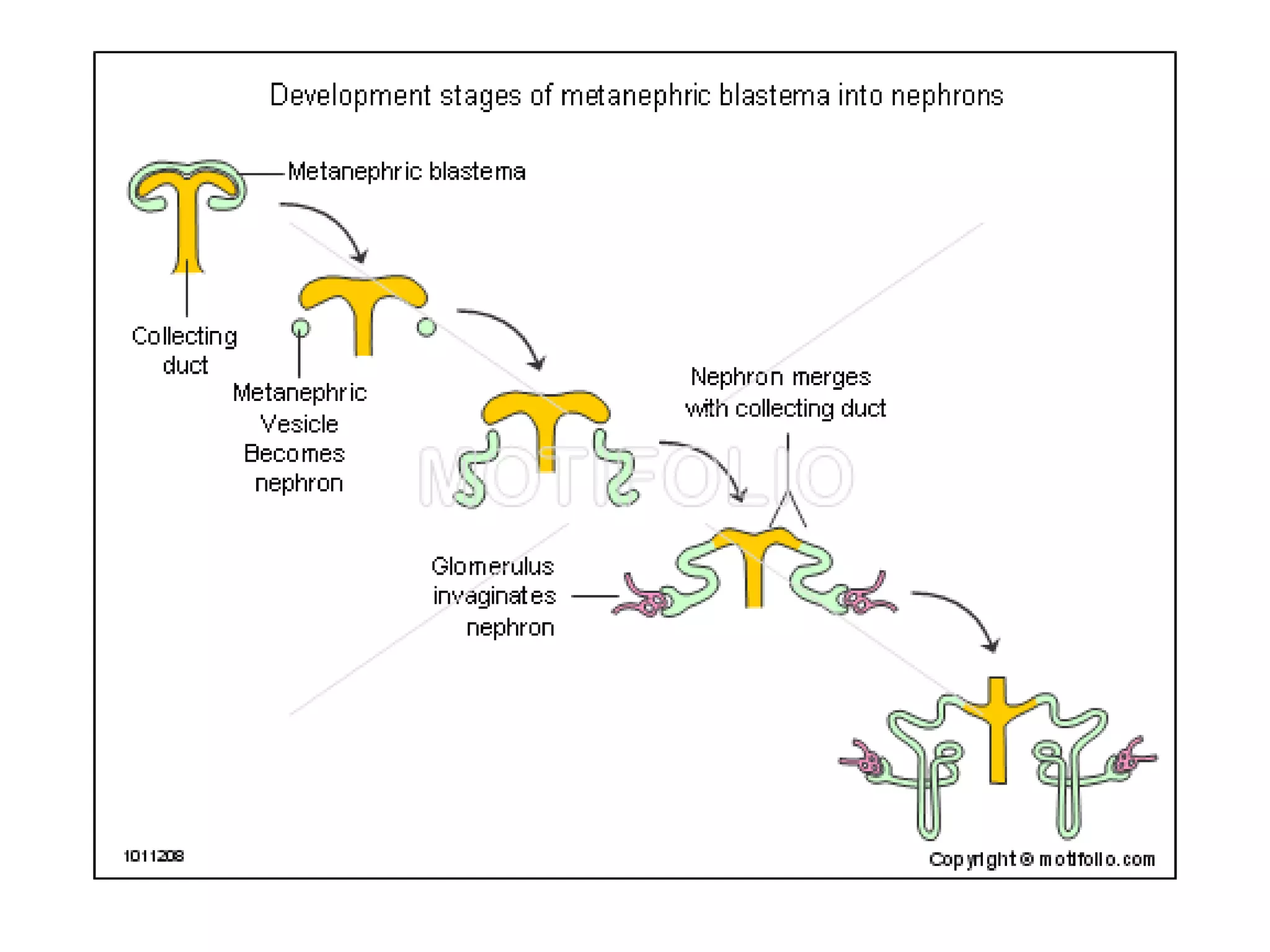
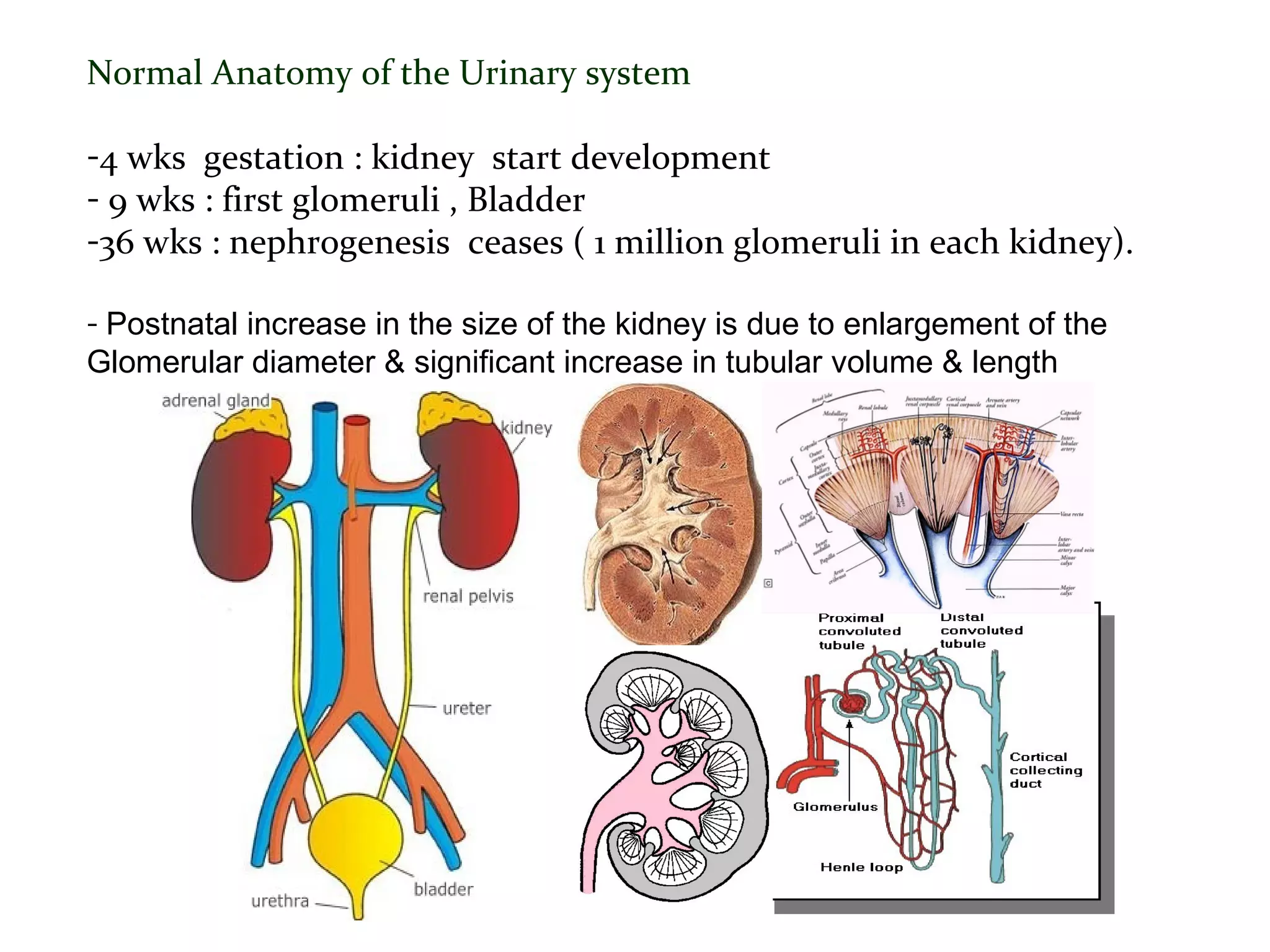
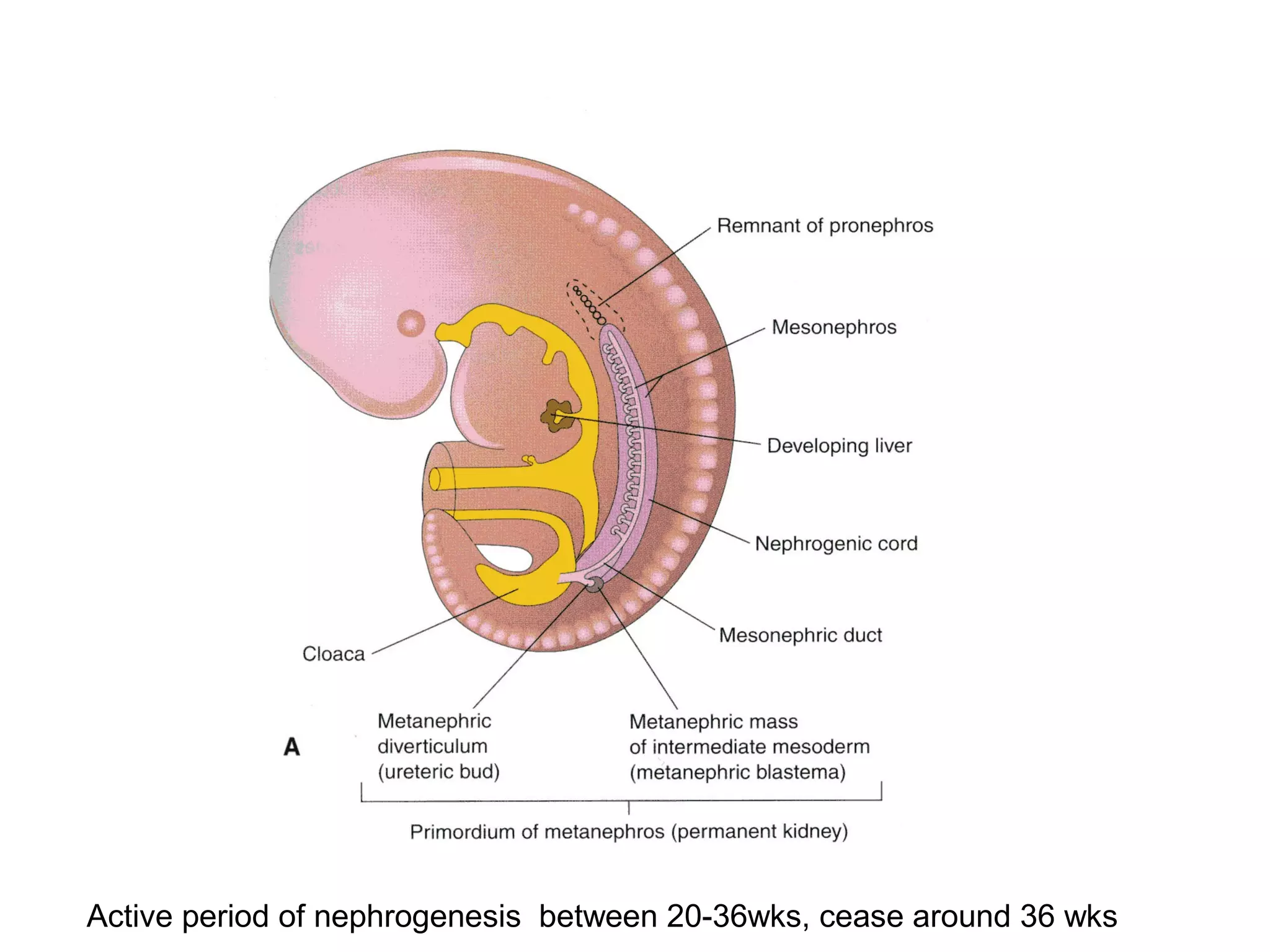
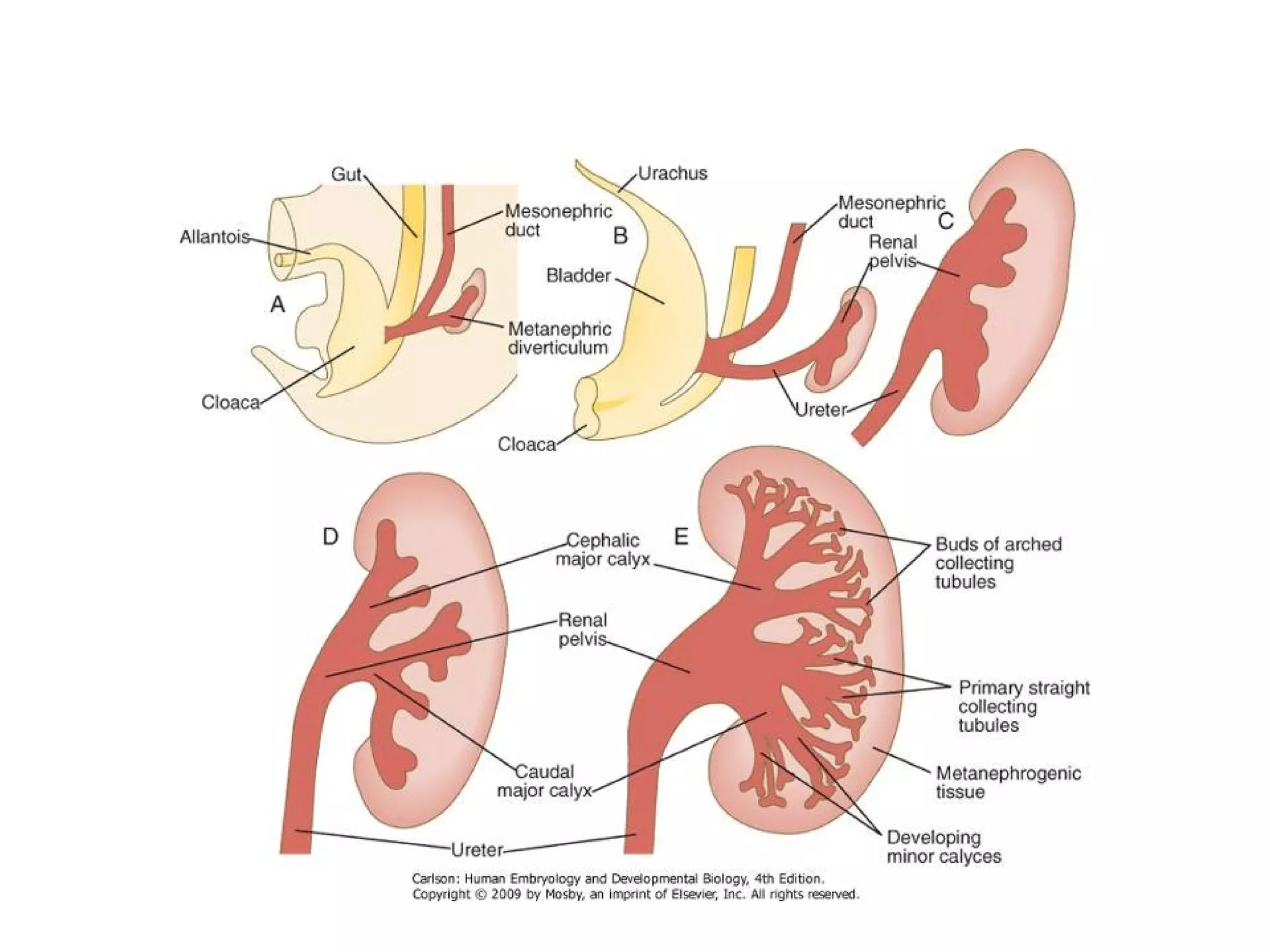
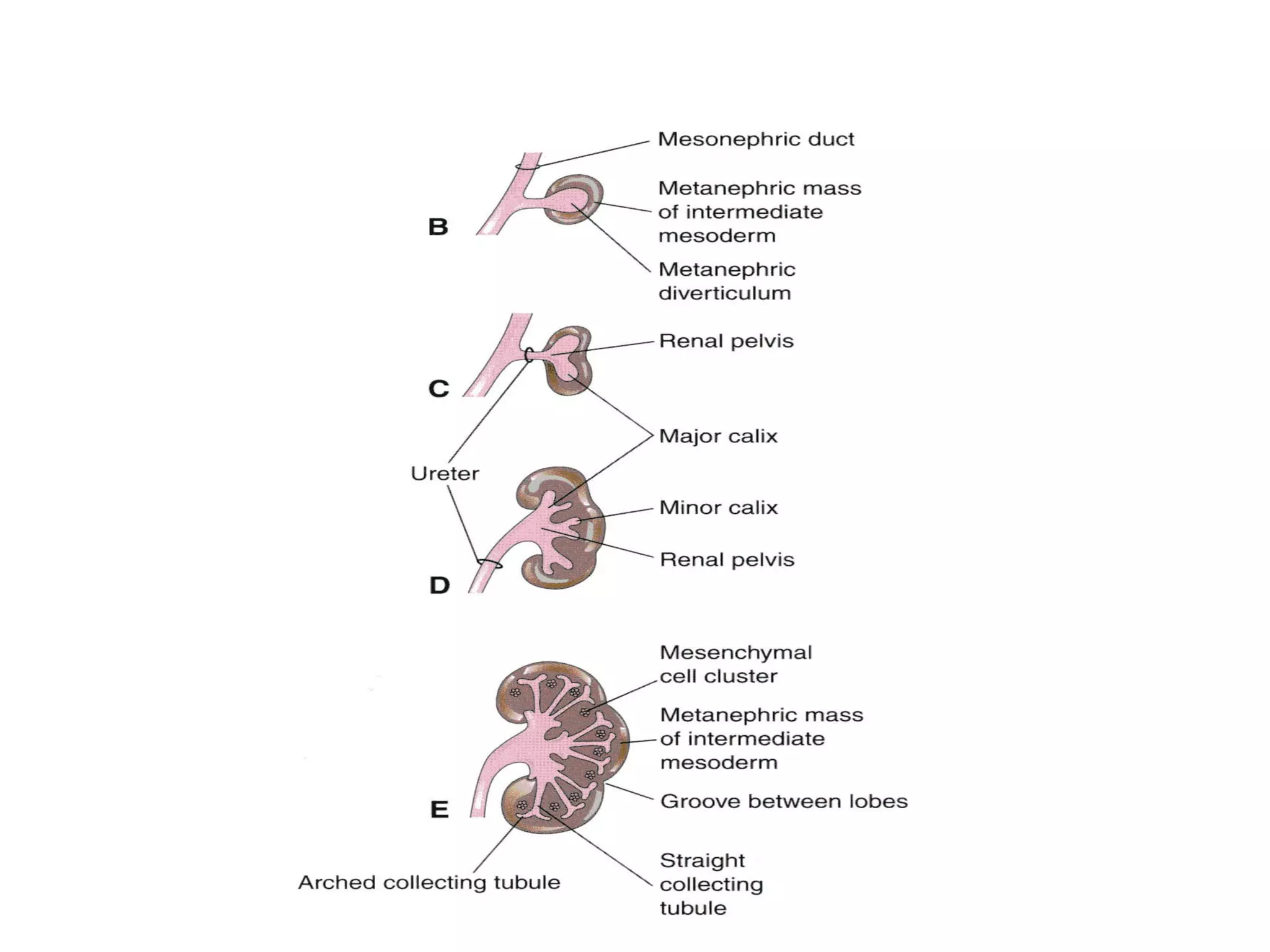
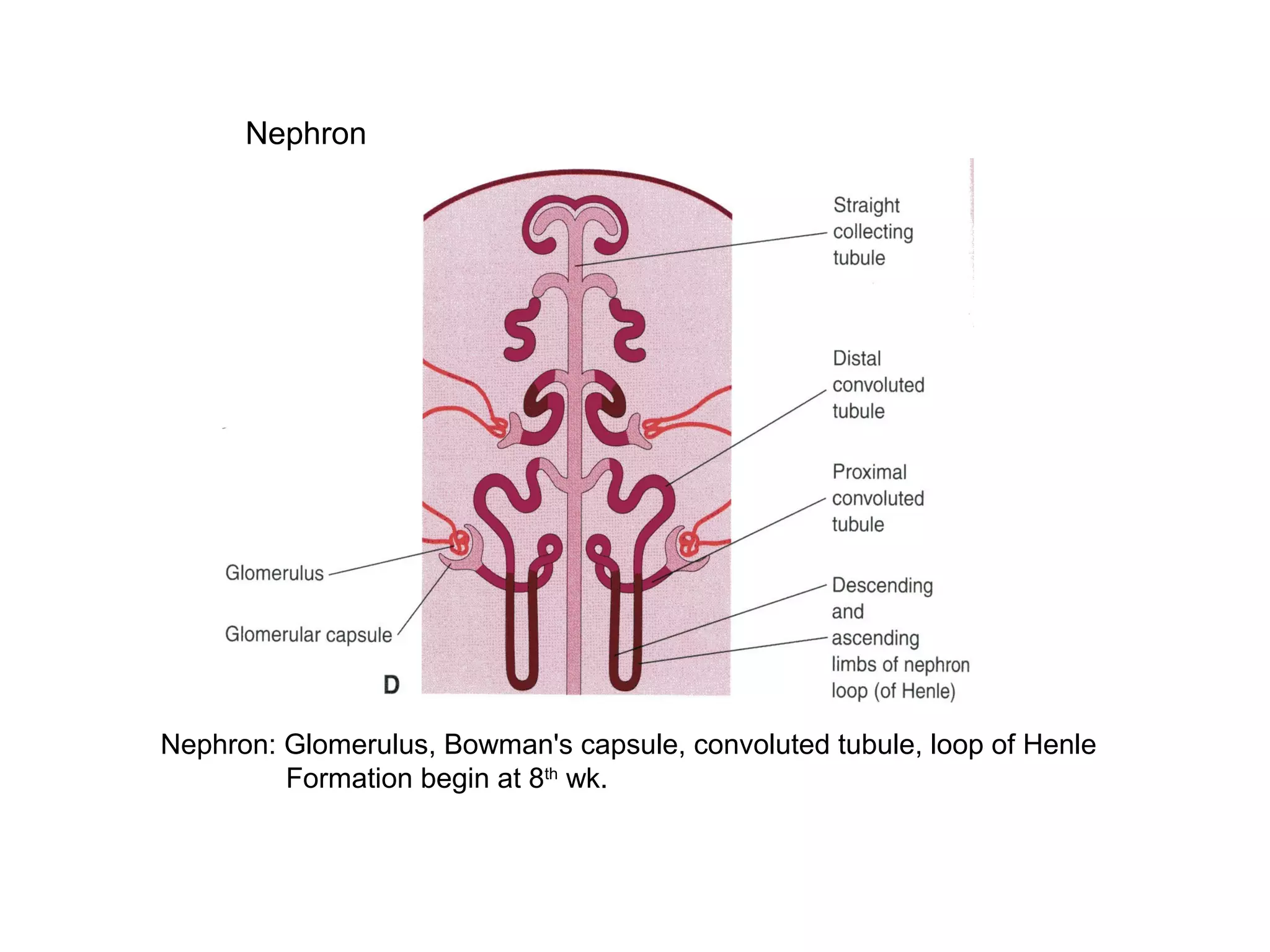
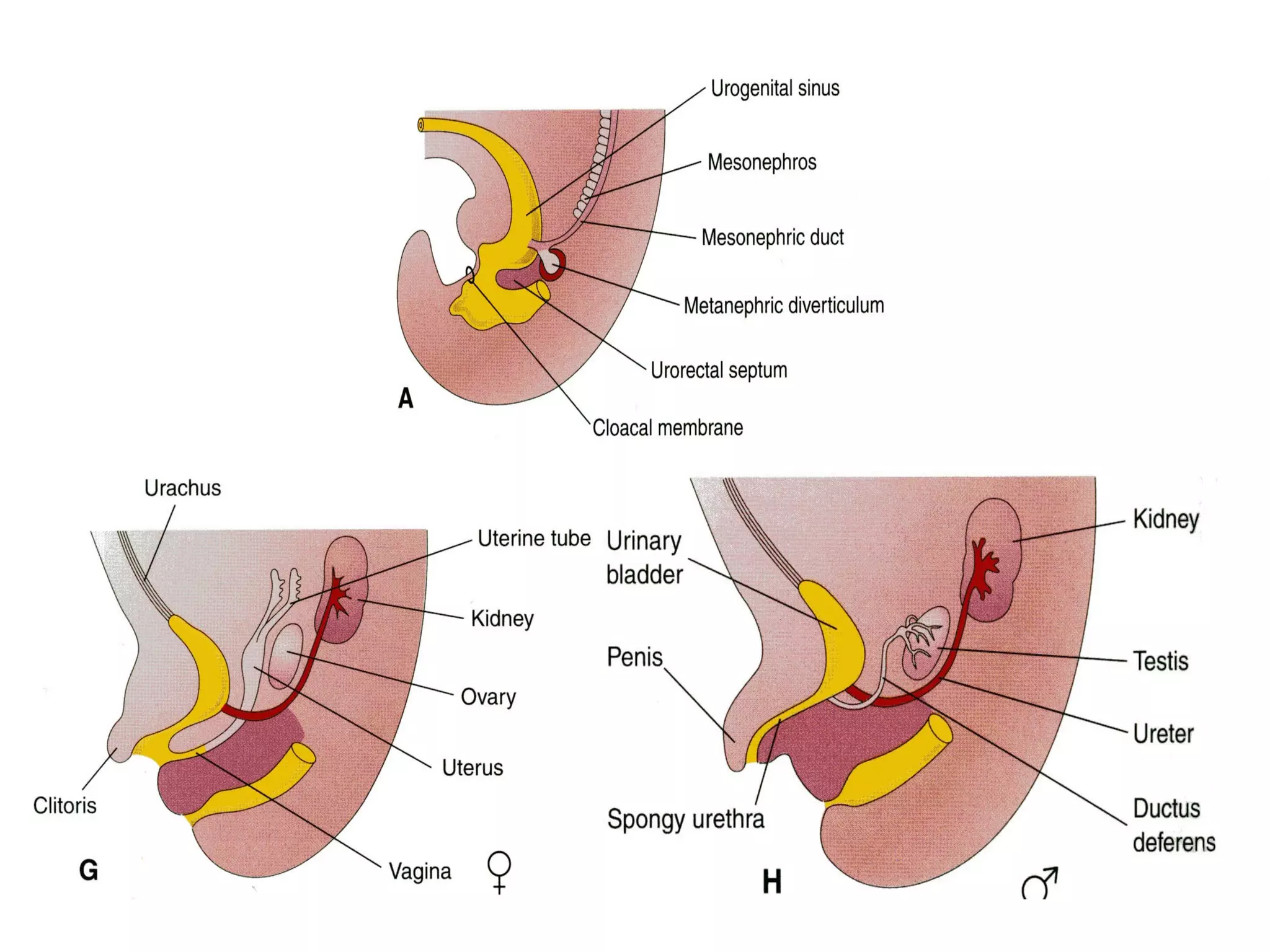
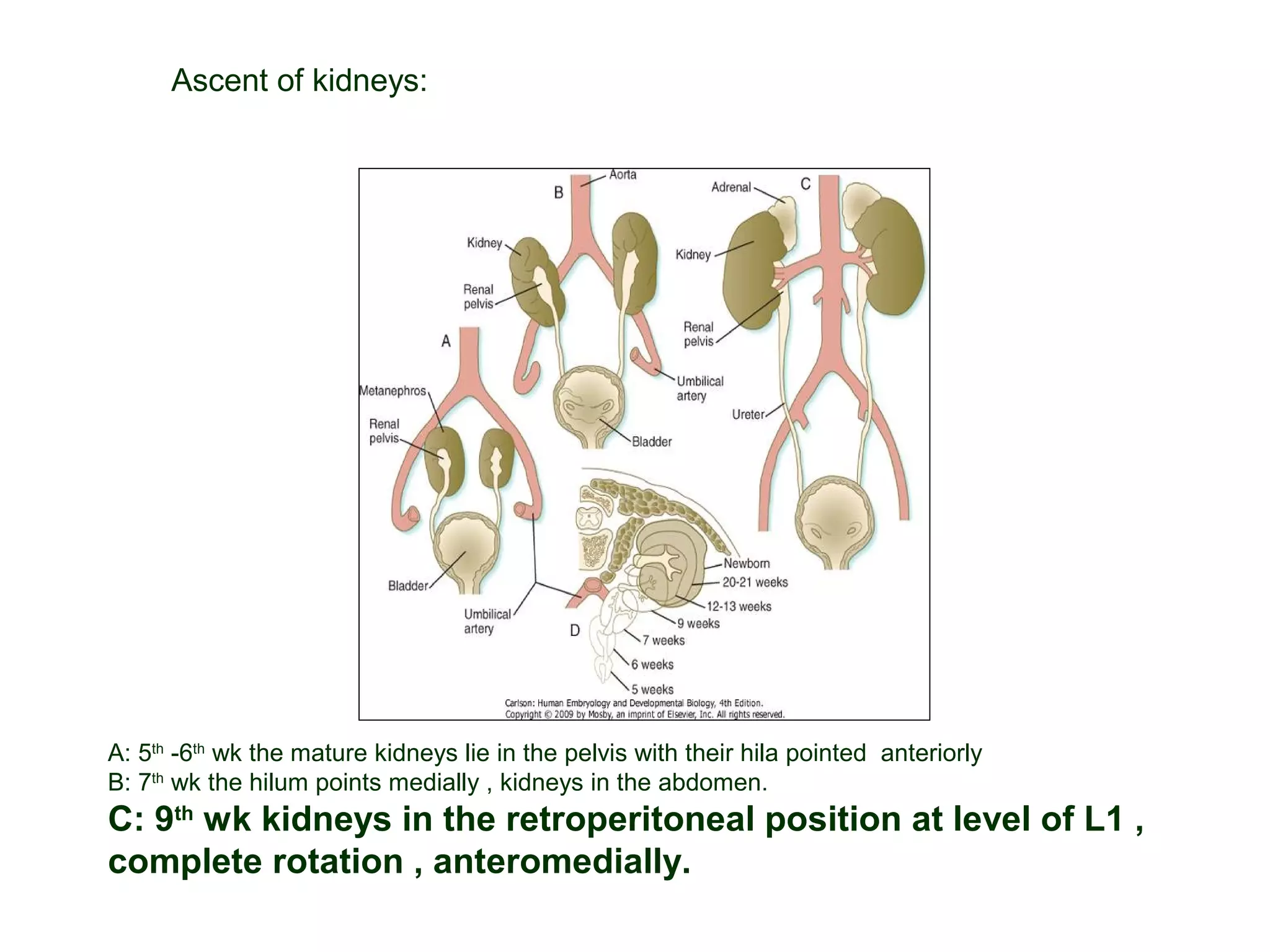
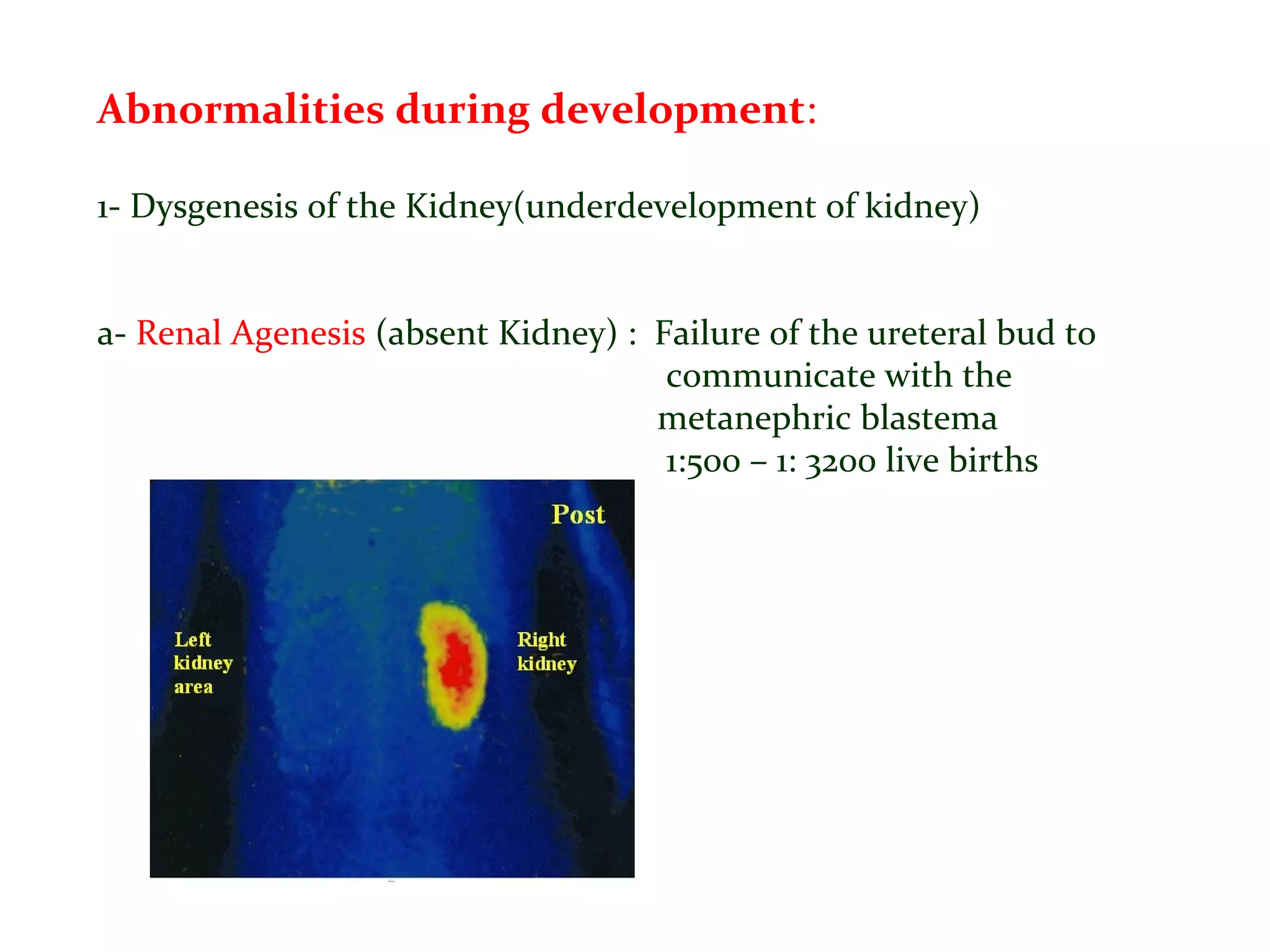
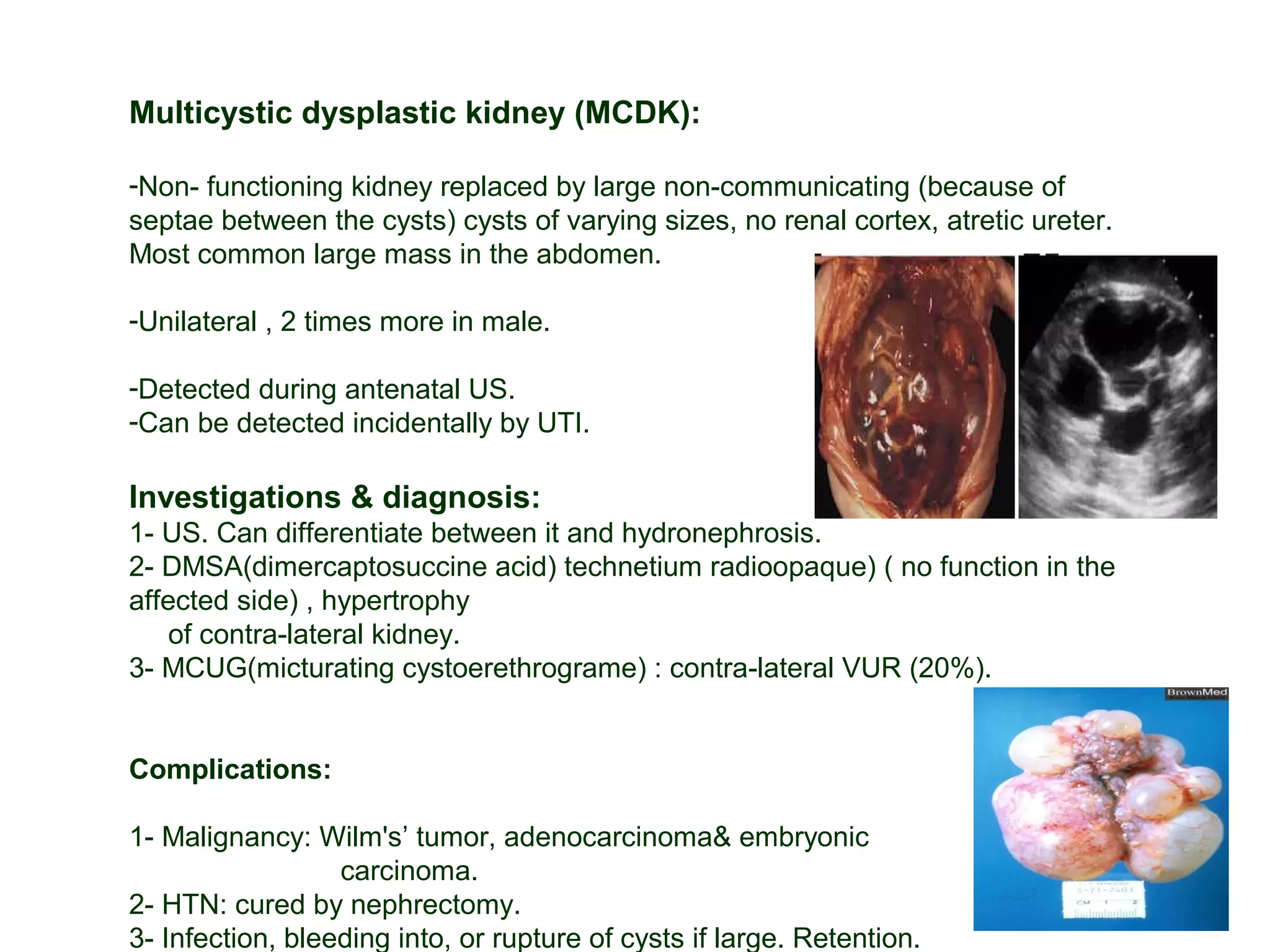
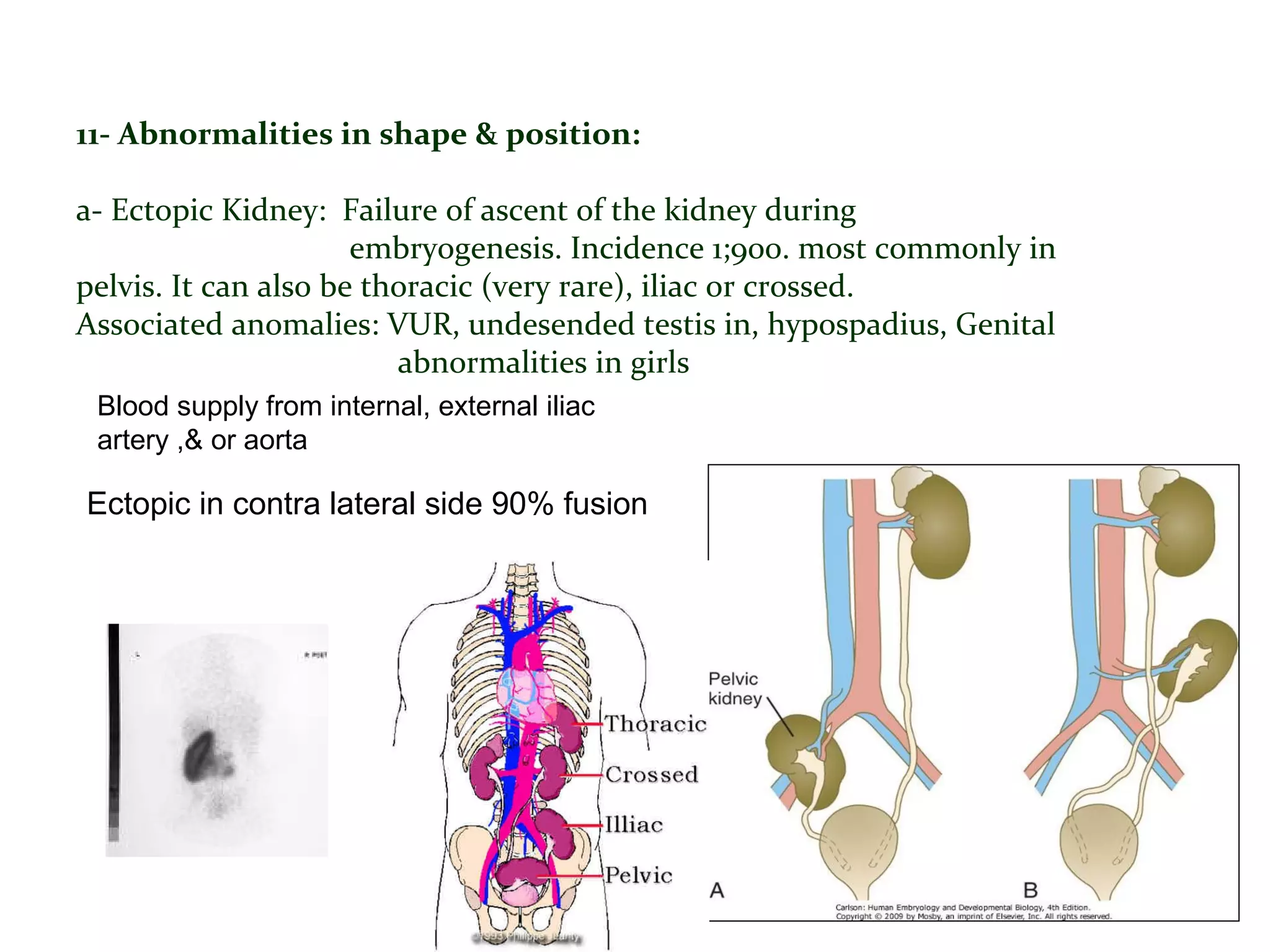

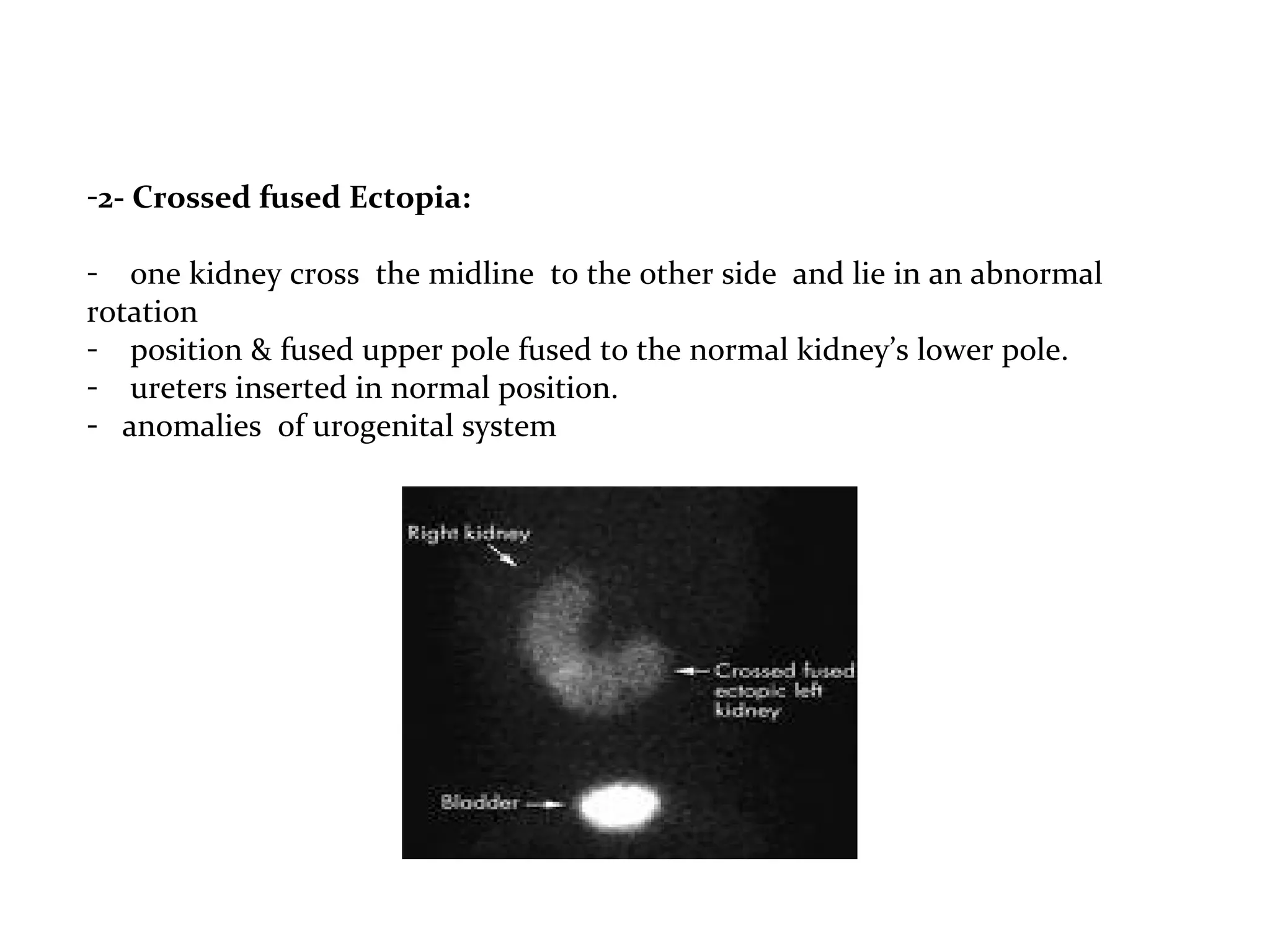

The document discusses congenital anomalies of the kidney and urinary system, covering normal development, anatomy, and various congenital disorders such as renal agenesis, dysplasia, and bladder extrophy. It details the embryologic phases of kidney development, common abnormalities, clinical presentations, diagnosis methods, and management strategies for affected individuals. It emphasizes the importance of early detection and ongoing follow-up for patients with these conditions.























































































