Downloaded 235 times



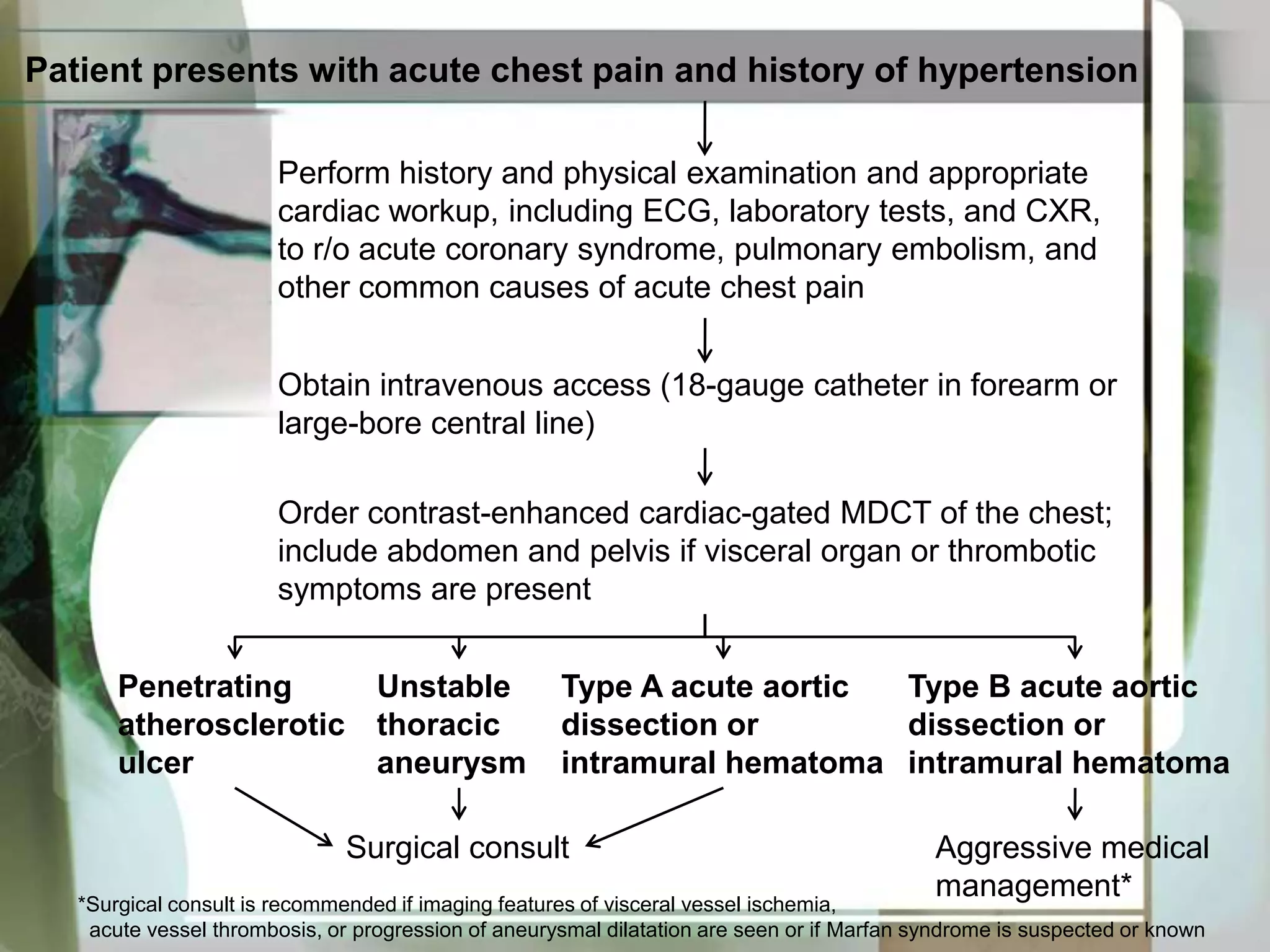














Contrast-enhanced, cardiac-gated CT is highly accurate for determining the cause of acute aortic syndrome, which can be due to aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, or unstable thoracic aneurysm. CT accurately identifies the location and extent of disease and guides urgent surgical or endovascular repair when needed to treat life-threatening conditions such as type A aortic dissection or ruptured aneurysm.






































































































