This document discusses stroke, including its types, causes, pathophysiology, imaging findings, and clinical features. It provides the following key points:
1. Stroke is caused by ischemia or hemorrhage in the brain. The main types are cerebral infarction (80%), intracerebral hemorrhage (15%), and subarachnoid hemorrhage (5%).
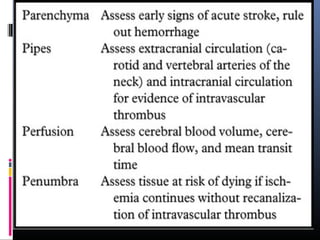
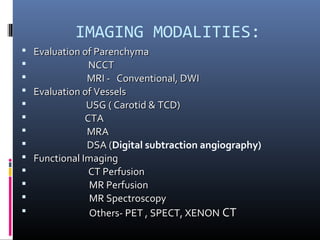
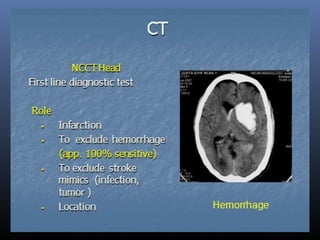
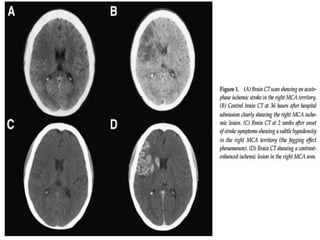
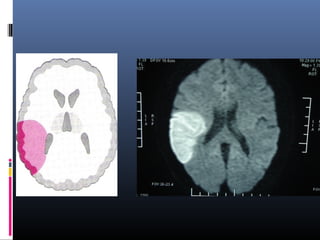
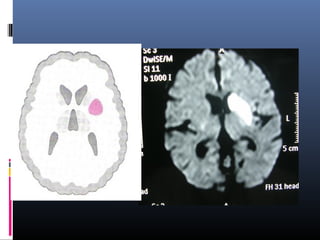
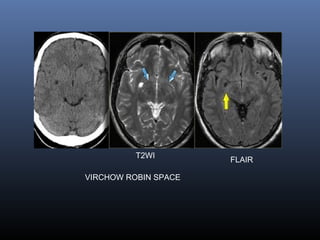
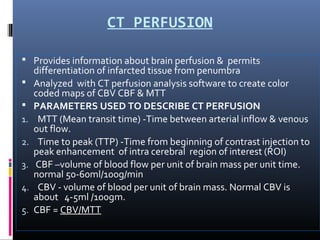
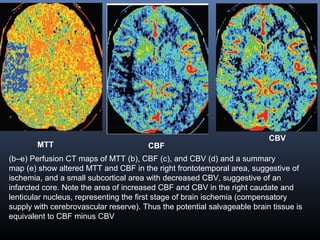
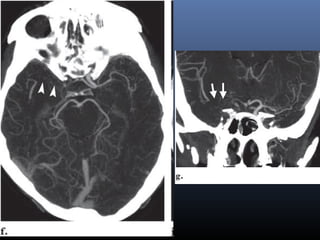
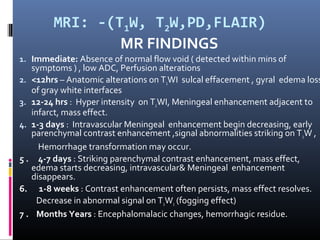
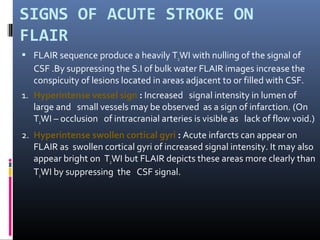
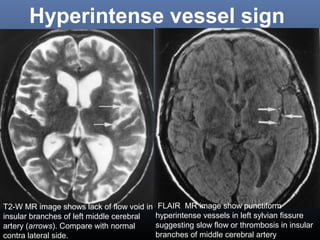
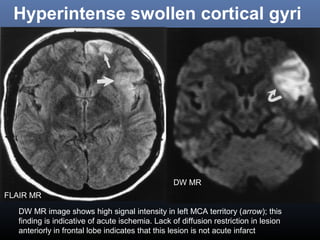
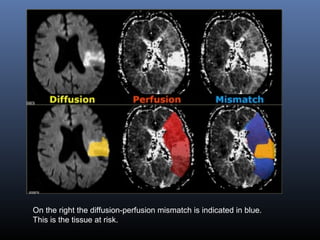
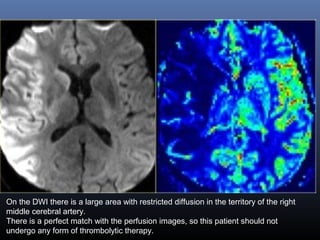
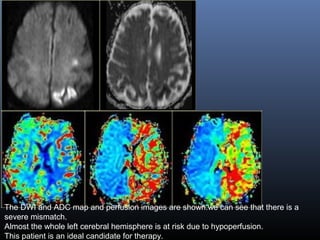
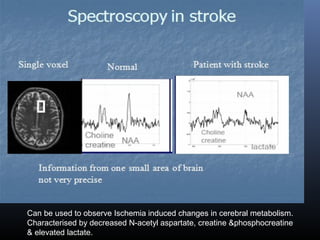
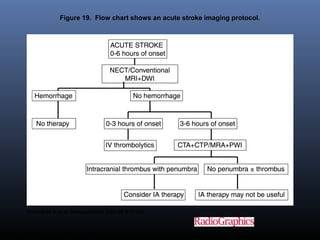
2. Imaging plays an important role in assessing the parenchyma, vessels, perfusion, and penumbra to guide therapy and predict outcomes. Techniques include CT, MRI, CT/MR perfusion, and angiography.
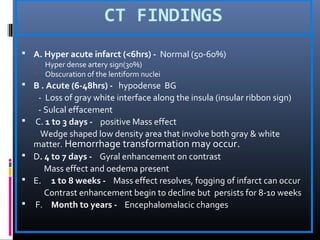
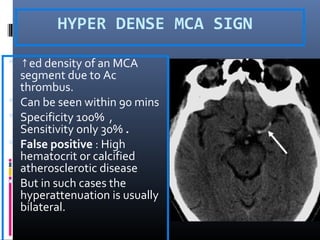
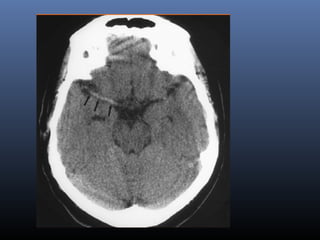
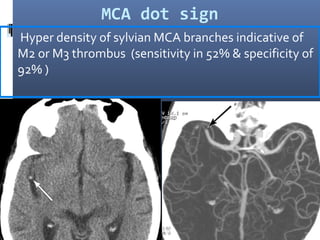
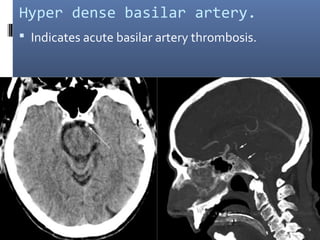
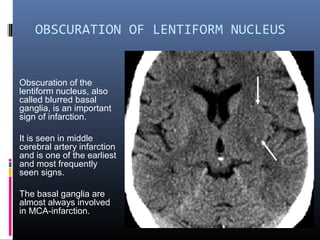
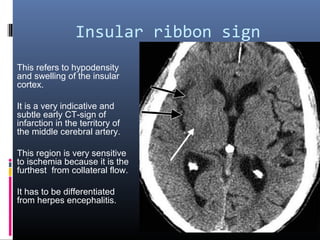
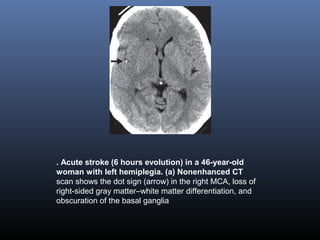
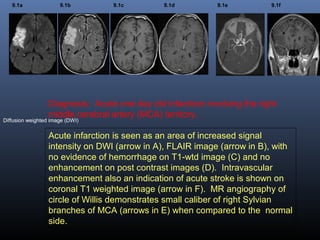
3. CT findings evolve over time from hyperacute to chronic stages. Early signs include