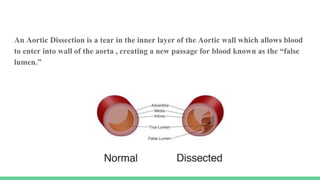
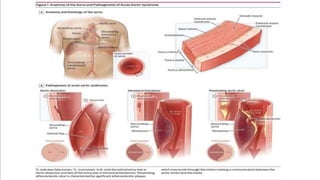
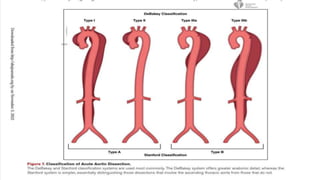
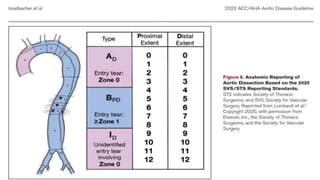
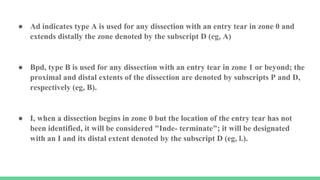
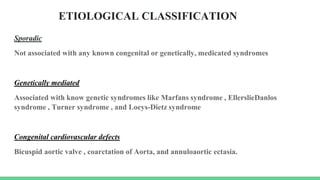
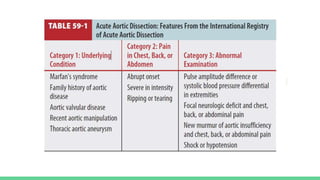
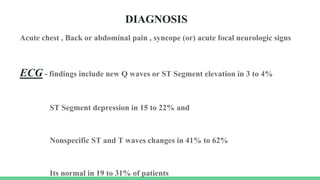
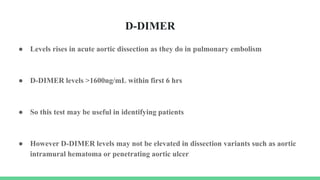
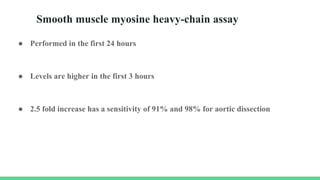
The document discusses aortic dissection, including its causes, risk factors, symptoms, diagnosis, and treatment. It defines aortic dissection as a tear in the inner layer of the aortic wall that allows blood to enter and dissect between the layers. It can cause problems like decreased blood flow or aortic rupture. Diagnosis involves tests like CT scans, echocardiograms, and blood markers. Treatment depends on the location of the dissection and may involve antihypertensive drugs or urgent surgery to repair the aorta.