
More Related Content
What's hot
What's hot (20)
Similar to Triple Rule Out Computed Tomography
Similar to Triple Rule Out Computed Tomography (20)
Recently uploaded
Recently uploaded (20)
Triple Rule Out Computed Tomography
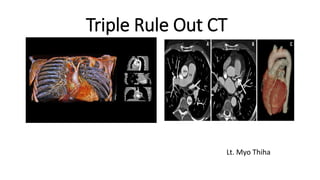
- 1. Triple Rule Out CT Lt. Myo Thiha
- 2. Objective To assess the validity and efficacy of Triple-rule-out (TRO) computed tomographic (CT) angiography in diagnosis of different vascular causes of chest pain.
- 3. Triple Rule Out CT TRO-CTA is a specialized computed tomography (CT) imaging exam tailored to evaluate for pathology within the coronary arteries, pulmonary arteries, and the aorta in a single CT study, hence the name ‘triple-rule out’.
- 4. Why we take TRO-CT? Acute chest pain is the second most common presentation after abdominal pain in the emergency department. represents a major diagnostic challenge in emergency care as it has a broad differential diagnosis varying from benign causes to life-threatening conditions. TRO studies are most appropriate and cost-effective when there is a suspicion for acute coronary syndrome along with other diagnoses such as pulmonary embolism, acute aortic syndrome, or nonvascular disease in the thorax.
- 5. Most common causes of Chest Pain Acute Coronary Syndrome Pulmonary Embolism Acute Aortic Syndrome
- 6. Causes of Chest pain Heart related causes Heart-attack Angina Aortic Dissection Digestive Causes Chest pain can be caused by disorders of the digestive system, including: Heartburn Swallowing disorders Gallbladder or pancreas problems
- 7. Muscle and bone causes Some types of chest pain are associated with injuries and other problems affecting the structures that make up the chest wall, including: Costochondritis Injured rib Lung-related causes lung disorders can cause chest pain, including: Pulmonary embolism Pleurisy Pulmonary hypertension
- 8. In many clinical situations, a definite diagnosis of ED chest pain is not possible solely based on clinical symptoms and laboratory findings. In addition, most diagnostic modalities (i.e., ECG, cardiac enzymes, exercise treadmill testing, radionuclide perfusion imaging and stress echocardiography) other than MDCT are focused on the diagnosis or exclusion of ACS and do not exclude other life-threatening causes of acute chest pain.
- 9. For this reason, Triple Role Out (TRO) protocol with ECG-gating technology has been proposed to encompass the entire thorax, allowing simultaneous evaluation of coronary arteries, thoracic aorta and pulmonary arteries for improving diagnosis of acute chest pain in a single study.
- 10. Criteria for TRO_CT study Clinical presentation – low to moderate risk of ACS Clinical presentation – non ACS diagnosed considered Normal ECG or non-specific changes Patient able to tolerate CT and hold breath Cardiac rhythm acceptable ECG gated scan Adequate renal function
- 11. Exclusion criteria Contra-indications to iodinated contrast material including known allergy and renal insufficiency (serum creatinine more than 1.4 mg/dl). Marked heart failure. Clinically unfit patients (unable to stop breathing during the examination). Extensive calcium score above 1000.
- 12. Why don’t we take coronary angiography above 1000 calcium score? Because of blooming artifacts, which can cause erroneous enlargement of calcification, make less accuracy to determine the coronary arteries lumen that results in false positive diagnosis. Fig: (A) shows enlargement in the lumen of RCA because of the blooming artifacts (B) shows normal in state of RCA
- 13. Anatomy of Aorta, Pulmonary and Coronary Aorta the largest blood vessel in the body. responsible for transporting oxygen rich blood from your heart to the rest of the body. begins at the left ventricle of the heart, extending upward into the chest to form an arch. downward into the abdomen, where it branches into the iliac arteries just above the pelvis.
- 14. Aortic Root the portion of the aorta that is attached to the heart. major part of the aortic root is the aortic valve allows blood to flow from the heart to the rest of the body when it is open and prevents blood from flowing backwards into the heart when it is closed.
- 15. Ascending Aorta begins at the sinotubular junction of the aortic root and extends up and out from the heart until it connects with the aortic arch.
- 16. Aortic Arch the portion of the aorta that is in the shape of an arch and connects the ascending aorta with the descending aorta. The major arteries : the brachiocephalic artery, the left carotid artery and the left subclavian artery.
- 17. Descending Thoracic Aorta begins at the end of the aortic arch and continues down into the abdomen. Two parts: 1. T. aorta(provides blood to the muscles of the chest wall and the spinal cord.) 2. Ab.Aorta (five arteries that branch from the abdominal aorta: the celiac artery, the superior mesenteric artery, the inferior mesenteric artery, the renal arteries and the iliac arteries)
- 18. celiac artery superior mesenteric artery inferior mesenteric artery renal arteries iliac arteries Stomach Liver Pancreas supplies blood to the small intestine supplies blood to the large intestine blood to the kidneys as well as the muscles of the abdominal wall and the lower spinal cord blood to the legs and the organs in the pelvis. Figure: shows five arteries from the abdominal aorta and their blood supply
- 19. Thoracic aorta disease 1. aortic aneurysms and dissections, 2. atherosclerotic disease, 3. infections and 4. traumatic injuries. Note: Ruptured thoracic aortic aneurysms and aortic dissections represent life-threatening emergencies that require immediate medical attention. Thoracic aortic aneurysms affect approximately 15,000 people in the United States each year
- 20. Symptoms 1. Chest pain 2. Back pain 3. Hoarseness 4. Wheezing 5. Difficulty swallowing 6. Cough
- 21. The most common types of aortic aneurysms are thoracic and abdominal. In addition, the following can signal a more serious condition: 1. Sudden and severe chest pain 2. Fainting 3. Leg pain or numbness 4. Shortness of breath 5. Weakness
- 22. Coronary Artery heart is mostly supplied by the two coronary arteries which arise from the ascending aorta immediately above the aortic valve. coronary arteries and their branches run on the surface of the heart. RCA arise from the anterior aortic sinus of the ascending aorta immediately above the aortic valve. first runs forwards between the pulmonary trunk and the right auricle.
- 23. Then, it descends almost vertically enter the rt. Atrioventricular groove, the rt. anterior coronary sulcus. At the inferior border of the heart, it turns posteriorly and runs into the atrioventricular groove, after the posterior interventricular groove finally anastomosing with the LCA.
- 24. LCA arise from the left posterior aortic sinus of the ascending aorta, immediately above the aortic valve and enters the left between the pulmonary trunk and the left auricle. then divides into the anterior interventricular artery also know as left anterior descending artery which runs downwards in the anterior interventricular groove to the apex of the heart.
- 26. Clinical Correlation Angina Pectoris – since coronary arteries are narrowed, the blood supply to the cardiac muscles is reduced. As a result, on exertion, the patient feels moderately severe pain in region of the left pericardium last as long as 20 mins. Pain is often referred to the left shoulder and medial side of the arm and forearm. Angina pectoris pain occurs on exertion and relieved by rest.
- 27. Myocardial Infarction sudden block of the larger branches of either coronary artery usually leads to myocardial ischaemia followed by the myocardial necrosis (myocardial infarction). Part of the heart suffering from MI, stops functioning and often causes death. This condition is termed as the heart attack or coronary attack.
- 28. Clinical features of MI Sensation of pressure, sinking and pain in the chest that lasts longer than 30 minutes. Nausea (or) vomiting, sweating, shortness of breath, and tachycardia. Pain radiates to the medial side of the arm, forearm, and hand. Sometimes, it may be referred to jaw or neck.
- 29. Sites of coronary artery occlusion The three most common site of CAO are 1. Anterior interventricular artery or LAD (40-50%), 2. RCA (30-40%) 3. Circumflex branch of LCA (15-20%) NOTE: MI mostly occurs at rest whereas angina occurs on exertion.
- 30. Blood supply of the major coronary arteries The 2 main coronary arteries are the left main and right coronary arteries. Left main coronary artery (LMCA). The left main coronary artery supplies blood to the left side of the heart muscle (the left ventricle and left atrium). The left main coronary divides into branches: 1. The left anterior descending artery branches off the left coronary artery and supplies blood to the front of the left side of the heart. 2. The circumflex artery branches off the left coronary artery and encircles the heart muscle. This artery supplies blood to the outer side and back of the heart.
- 31. Right coronary artery (RCA) The right coronary artery supplies blood to the right ventricle, the right atrium, and the SA (sinoatrial) and AV (atrioventricular) nodes, which regulate the heart rhythm. The right coronary artery divides into smaller branches, including the right posterior descending artery and the acute marginal artery. Together with the left anterior descending artery, the right coronary artery helps supply blood to the middle or septum of the heart.
- 32. Fig: Coronary arteries and their blood supply
- 33. Fig: Coronary Arteries and their branches
- 34. Types of Circulation Pulmonary Circulation the portion of the cardiovascular system that carries oxygen-poor (deoxygenated) blood from the heart to the lungs and returns oxygenated blood back to the heart. deoxygenated blood from the body leaves the right ventricle through the pulmonary arteries, which carry the blood to each lung. 34
- 35. Cont.; pulmonary arteries are the only arteries that carry deoxygenated blood. In the lungs, red blood cells release carbon dioxide and pick up oxygen during respiration. The oxygenated blood then leaves the lungs through the pulmonary veins, which return it to the left side of the heart and complete the pulmonary cycle.
- 36. Cont.; The oxygenated blood is then distributed to the body through the systemic circulation before returning again to the pulmonary circulation.
- 37. Fig: The pulmonary circulation carries blood between the heart and lungs.
- 38. Systemic Circulation the portion of the cardiovascular system that carries oxygenated blood from the heart to the body and returns deoxygenated blood back to the heart. Oxygenated blood from the lungs leaves the left ventricle through the aorta. From here it is distributed to the body's organs and tissues, which absorb the oxygen through a complex network of arteries, arterioles, and capillaries.
- 39. Cont.; The deoxygenated blood is then collected by venules and flows into veins before reaching the inferior and superior venae cavae, which return it to the right heart, completing the systemic cycle. The blood is then re-oxygenated through the pulmonary circulation before returning again to the systemic circulation.
- 40. Fig: The systemic circulation. The systemic circulation brings oxygenated blood to the body cells and tissues and transports cellular wastes away from the cells and tissues. It is also responsible for temperature regulation and transport of hormones and other substances around the body.
- 41. Coronary Circulation the heart needs its own blood supply, which it gets through the coronary circulation. the heart muscle tissue is so thick that it needs blood vessels to deliver oxygen and nutrients deep within it. The vessels that deliver oxygen-rich blood to the heart muscle are called coronary arteries.
- 42. Cont.; branch directly from the aorta, just above the heart. The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins.
- 44. Patient preparation for TRO An 18–20-gauge intravenous catheter is placed into a large vein in the antecubital fossa. The patient is lying in a supine position with arm in front of him. ECG leads are positioned above and below the level of the scan to prevent streak artifact. The ideal heart rate for ECG-gated studies is a slow regular rhythm, usually a sinus bradycardia at 50–60 beats per minute. Oral-blockers may be given at least 1 h before the scan for control of heart rate.
- 45. Contrast material and scanning protocol In order to image both the coronary and pulmonary arteries, a biphasic injection technique was used: 70 mL of undiluted (ultravist 370) was injected at 5 mL/s, followed by 25 mL of the same contrast material diluted with 25 mL of saline, also injected at 5 mL/s. For injection Protocol we used a bolus tracking technique where we started contrast medium injection when the HU in the left atrium reached 100 HU then in the second phase we depended on the observation, for assessment of the opacification of the pulmonary artery.
- 46. The first phase of the injection opacifies the coronary arteries during image acquisition, while the second phase of the injection, provides simultaneous homogeneous enhancement of the pulmonary arteries. Data acquisition starts from the level of the medial end of the clavicles to the lower border of the heart in cranio–caudal direction.
- 47. Fig: Typical Z axis coverage in dedicated coronary CT angiography versus triple rule-out study. A: the field of view in a dedicated coronary CT angiography is demonstrated. B: note the increased Z axis length in the triple rule-out study compared with dedicated coronary CT angiography.
- 48. Data evaluation For coronary assessment every case was evaluated in the axial plane and with slab maximum intensity projection images that were rotated to visualize each vessel in multiple planes. Vessels with complex plaque were also evaluated with curved multiplanar reconstruction by using vessel tracking software with automatic centerline determination.
- 49. Different parts of the thoracic aorta regarding their diameter, contrast filling, presence of filling defects, dissections, wall irregularities, calcification, mural thrombus. The main pulmonary artery, right and left pulmonary arteries, their segmental and subsegmental branches, regarding their diameter, contrast filling, presence of filling defects, wall irregularities, calcification, mural thrombus.
- 50. Other extra-vascular structures such as cardiac size, pleural, pericardial and parenchymal abnormalities have to be assessed.
- 51. Female patient 37 year old presenting with acute chest pain, dyspnea and hemoptysis. CT axial (A and B), sagittal (C) and (D) images of pulmonary angiography showing left main and segmental pulmonary embolism and left sided pleural effusion.
- 52. Triple rule-out CT angiography images (sagittal and axial views) of two patients with aortic dissection, with standard (a, b) and low dose (c, d). The diagnostic and image quality were excellent in both patients in the left descending artery (white arrow), the aorta(white star) and the pulmonary artery (arrowhead). The first patient had an history of surgical replacement of the ascending aorta.
- 53. Pros TRO CT can reduce (a) time for patient triage, (b) number of required diagnostic tests, (c) costs, and (d) radiation exposure to the patient.
- 54. Limitations Beta-blockers that are required for coronary CTA may not be safe in patients with pulmonary embolism. Obesity and calcifications limit interpretation, rapid heart rate, arrhythmias, renal dysfunction and contrast allergies.
- 55. Conclusion Since there are a lot of chest pain cases in emergency department , it is difficult to know the real cause of chest pain. triple rule out is a relatively new technique, examination the coronary arteries, pulmonary arteries and aorta in just a single study, which gives us the advantage of screening emergency patients presenting with chest pain in a rapid and safe way for detection of their vascular diseases. In addition, it can reduce the radiation dose to the patient because it investigates the coronary arteries, pulmonary arteries and aorta in just a single study and we don’t need to separated studies to check those of them. That’s why, it is most effective investigation to know the origin of abnormalities even though it has still challenges.
- 56. References Pitts SR, Niska RW, Xu J, Burt CW. National hospital ambulatory medical care survey: 2006 emergency department summary. Natl Health Stat Rep 2008;7:1–8. Stillman AE, Oudkerk M, Ackerman M. Use of multidetector computed tomography for the assessment of acute chest pain: aconsensus statement of the North American Society of Cardiac Imaging and the European Society of Cardiac Radiology. Int J Cardiovascular Imaging 2007;23:415–27. Thomas J, Rideau AM, Paulson EK, Bisset 3rd GS. Emergency department imaging: current practice. J Am Coll Radiol 2008;5(7):811–816e2.
- 57. Kevin M, Ethan J. Evaluation of a ‘‘Triple Rule-Out’’ coronary CT angiography protocol: use of 64-section CT in low-tomoderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008;248(2). Rubinshtein R, Halon D, Gaspar T, et al. Usefulness of 64-slice cardiac computed tomographic angiography for diagnosing acute coronary syndromes and predicting clinical outcome in emergency department patients with chest pain of uncertain origin. Circulation 2007;115:1762–8. Kevin M, Ethan J. Evaluation of a ‘‘Triple Rule-Out’’ coronary CT angiography protocol: use of 64-section CT in low-tomoderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008;248(2)
- 58. THANK YOU