Download to read offline
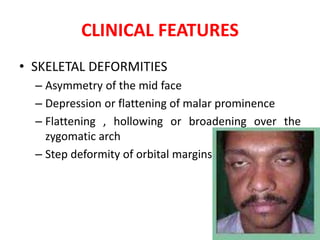
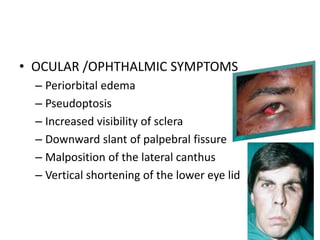
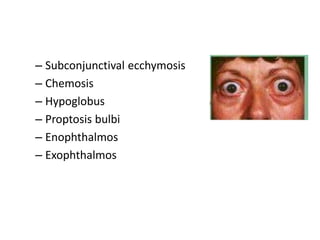
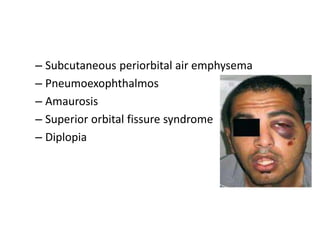


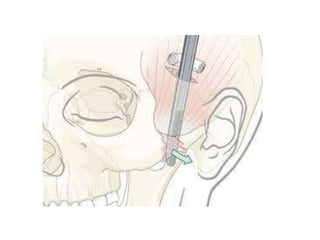

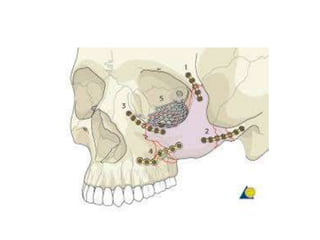

This document discusses the classification, clinical features, investigation, management, and complications of zygomatic bone fractures. It describes 8 types of zygomatic bone fractures classified by Row and Killey or Knight and Northwood. Clinical features include midface deformities, ocular symptoms like diplopia, neurological symptoms, oral symptoms like trismus, and nasal symptoms like epistaxis. Management involves surgical approaches like bicoronal or Gillies temporal to reduce the fracture using indirect or direct methods, then fixing with miniplates in 1-4 points. Complications can include infraorbital numbness, enophthalmos, diplopia, or superior orbital fissure syndrome.























































































