Downloaded 811 times

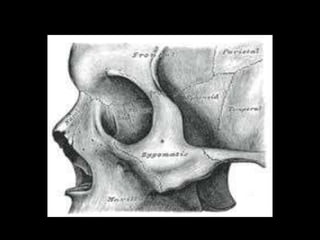
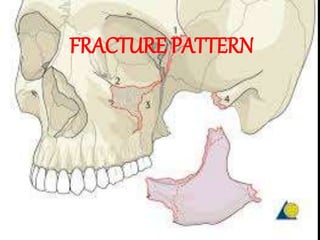


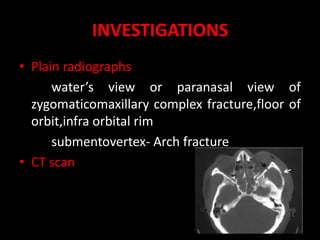
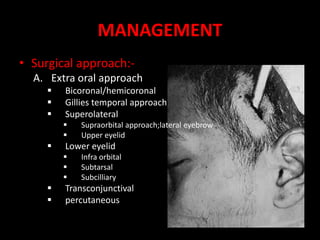
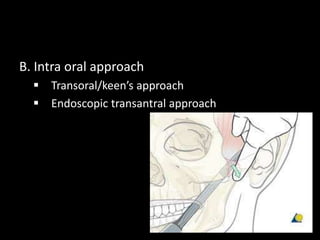
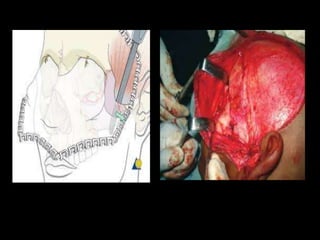
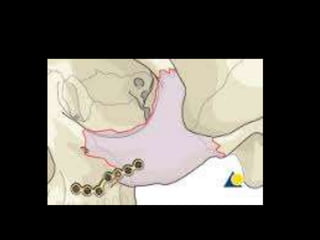
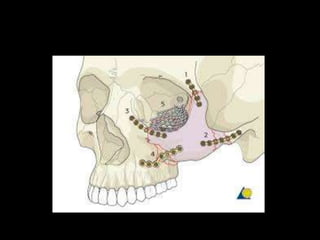

The document summarizes the zygomaticomaxillary complex fracture, including its anatomy, fracture patterns, classification systems, clinical features, investigations, management approaches, reduction techniques, fixation methods, and potential complications. Key points include that the fracture pattern typically involves 3 lines extending from the inferior orbital fissure in different directions, and management often involves open reduction and internal fixation using either a transoral/Keen's approach, Gillies temporal approach, or bicoronal approach depending on the fracture type and displacement. Complications can include nerve damage, malunion, enophthalmos, and infection.




















































































