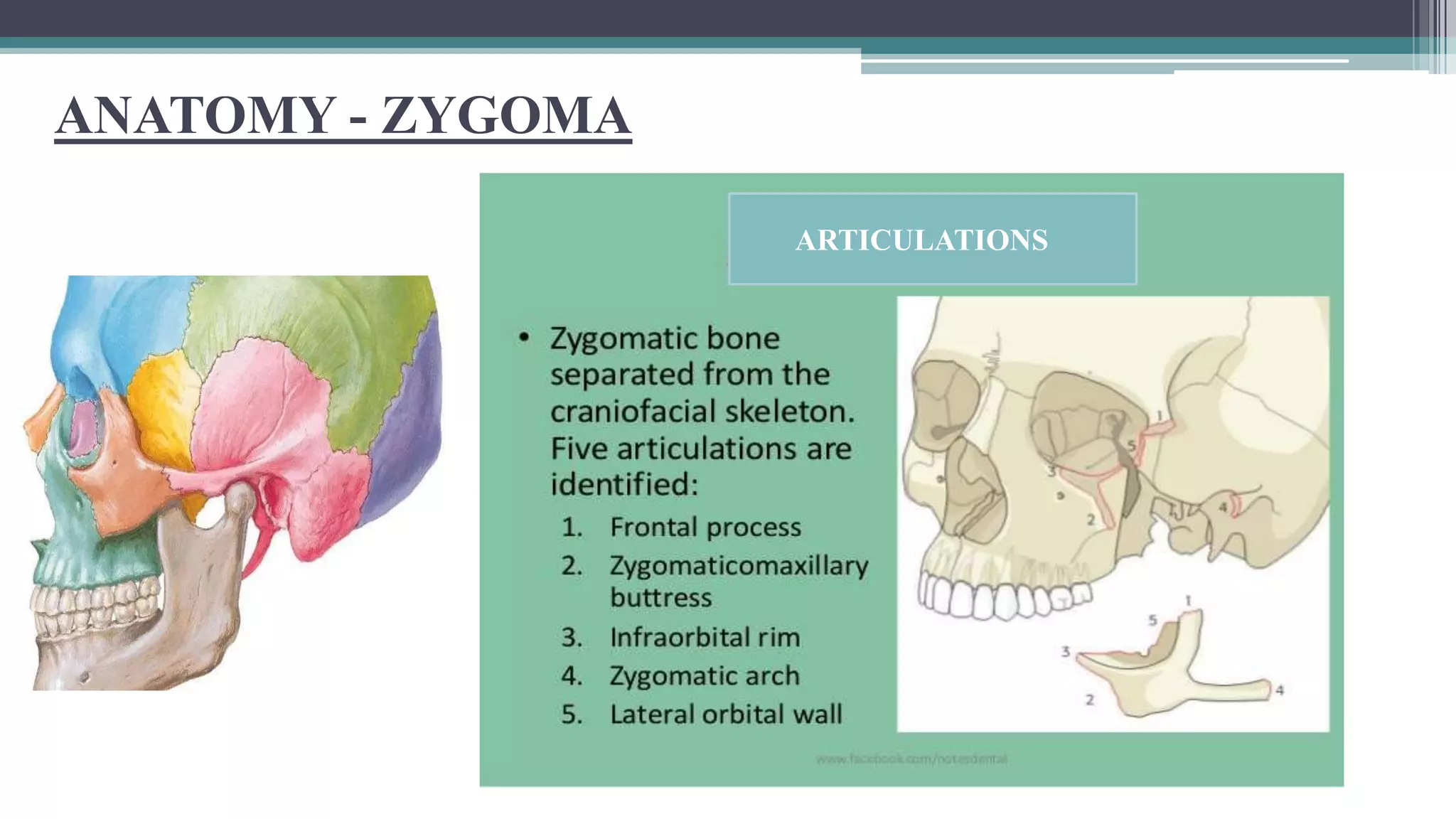
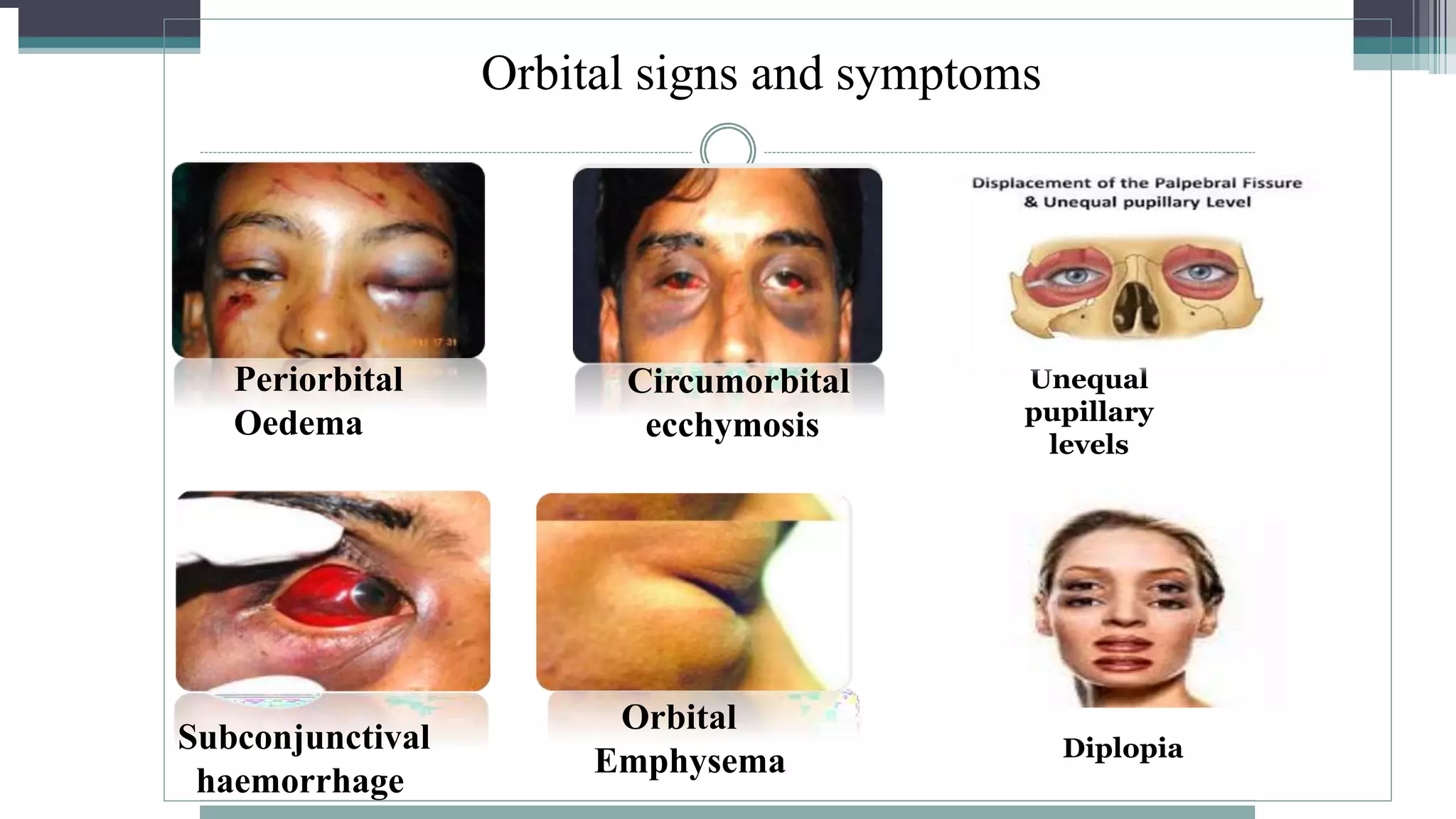
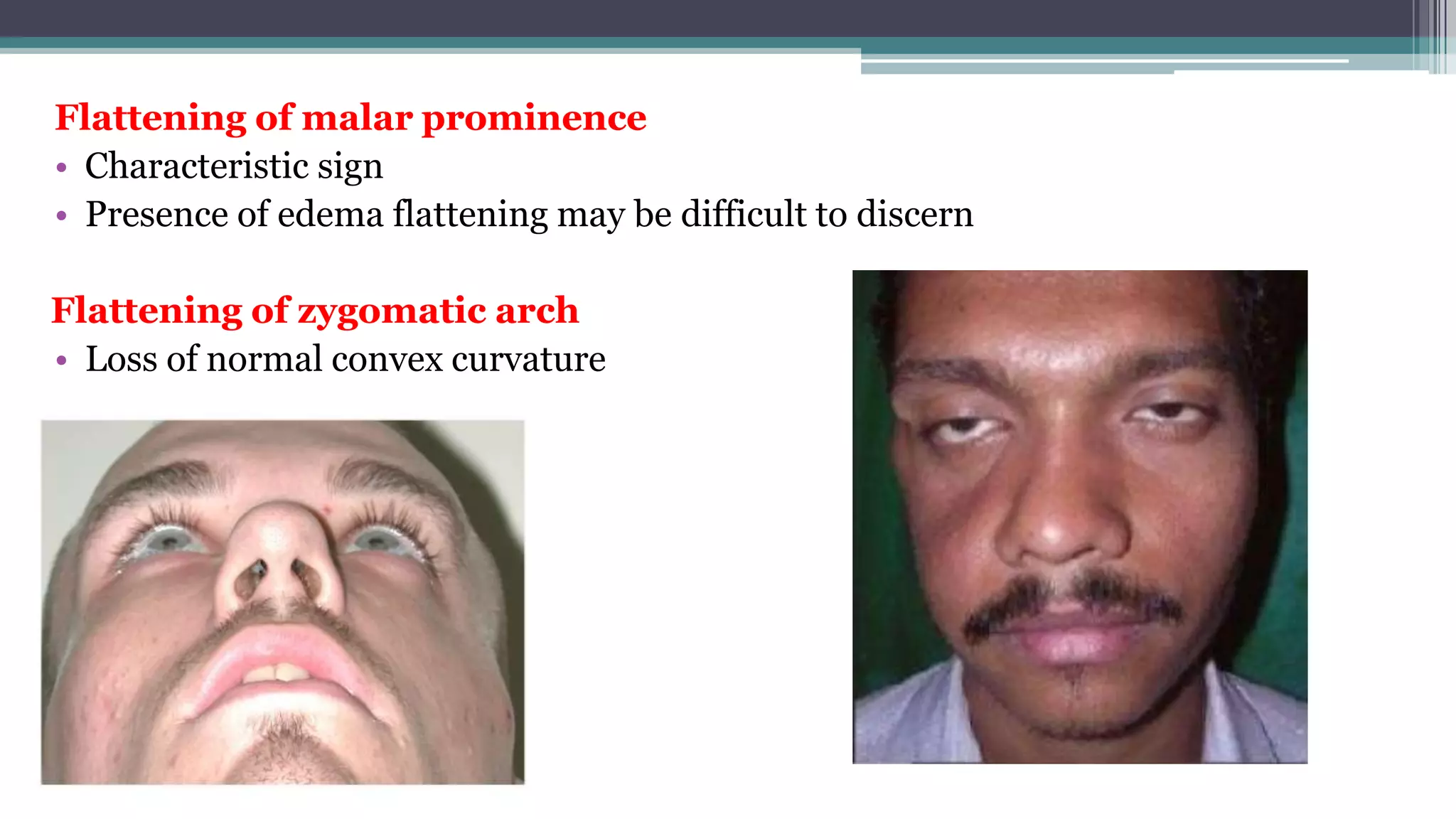
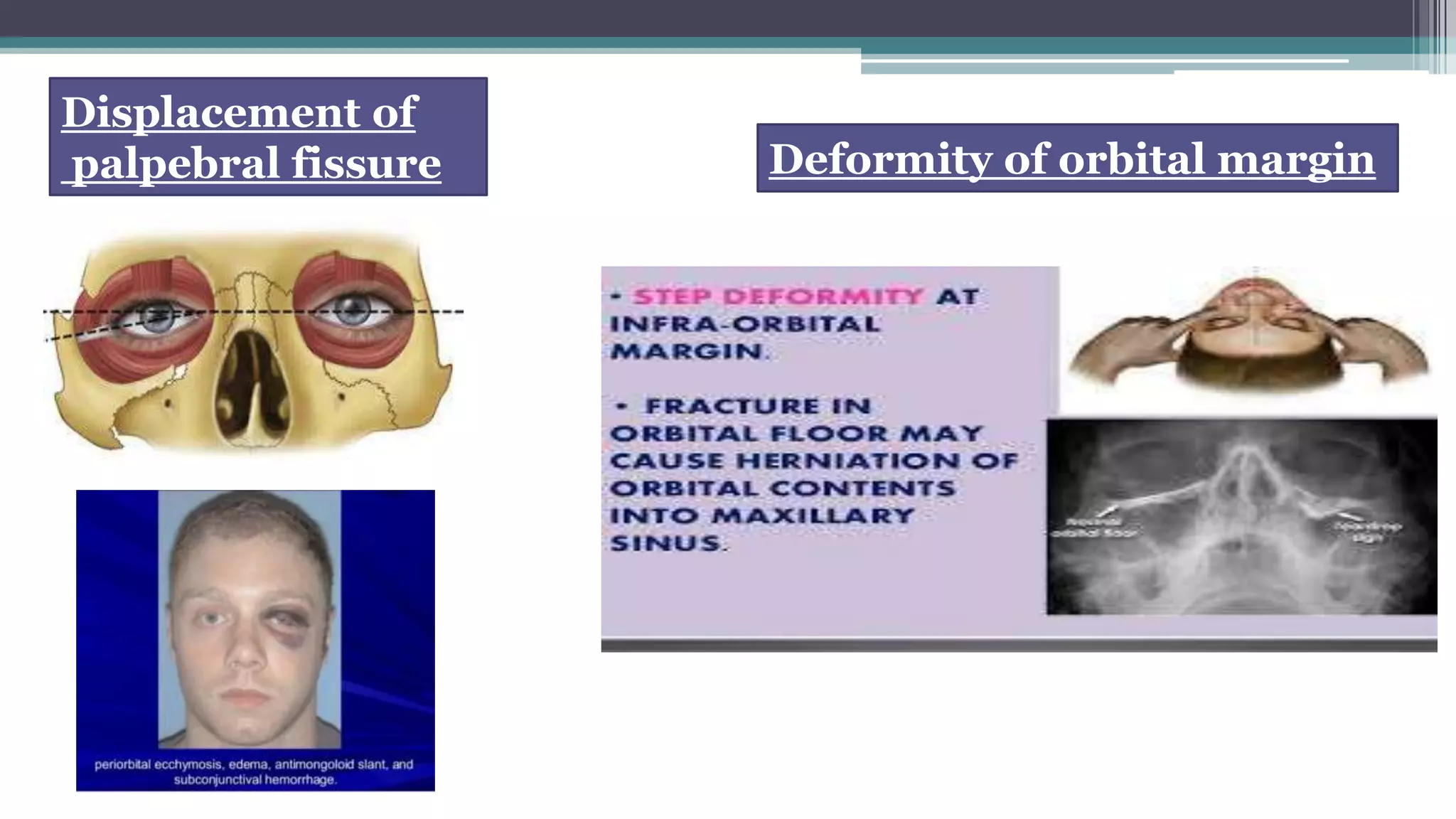
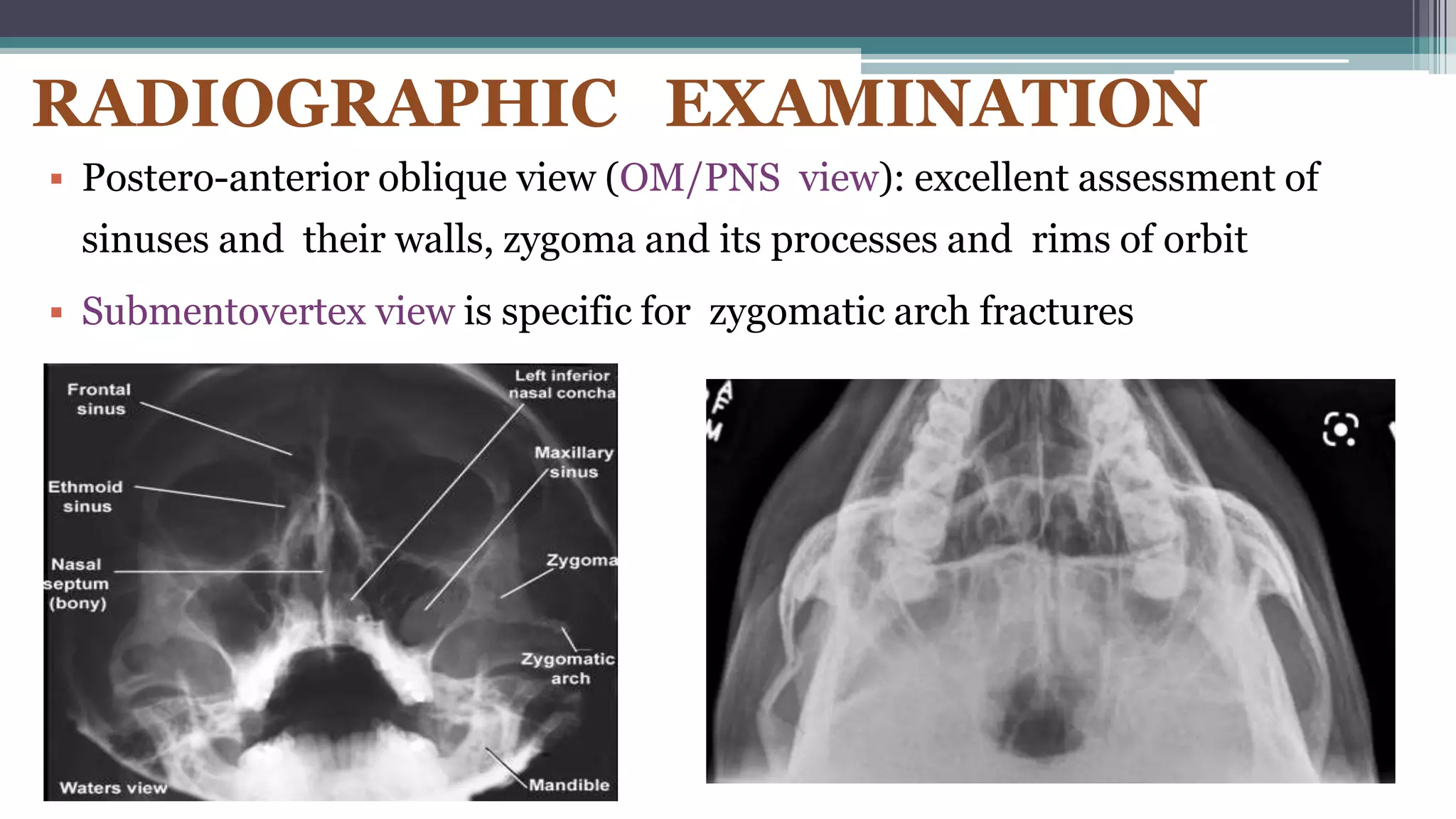
1) The document discusses zygomaticomaxillary fractures, providing classifications, examination techniques, signs and symptoms, and treatment approaches.
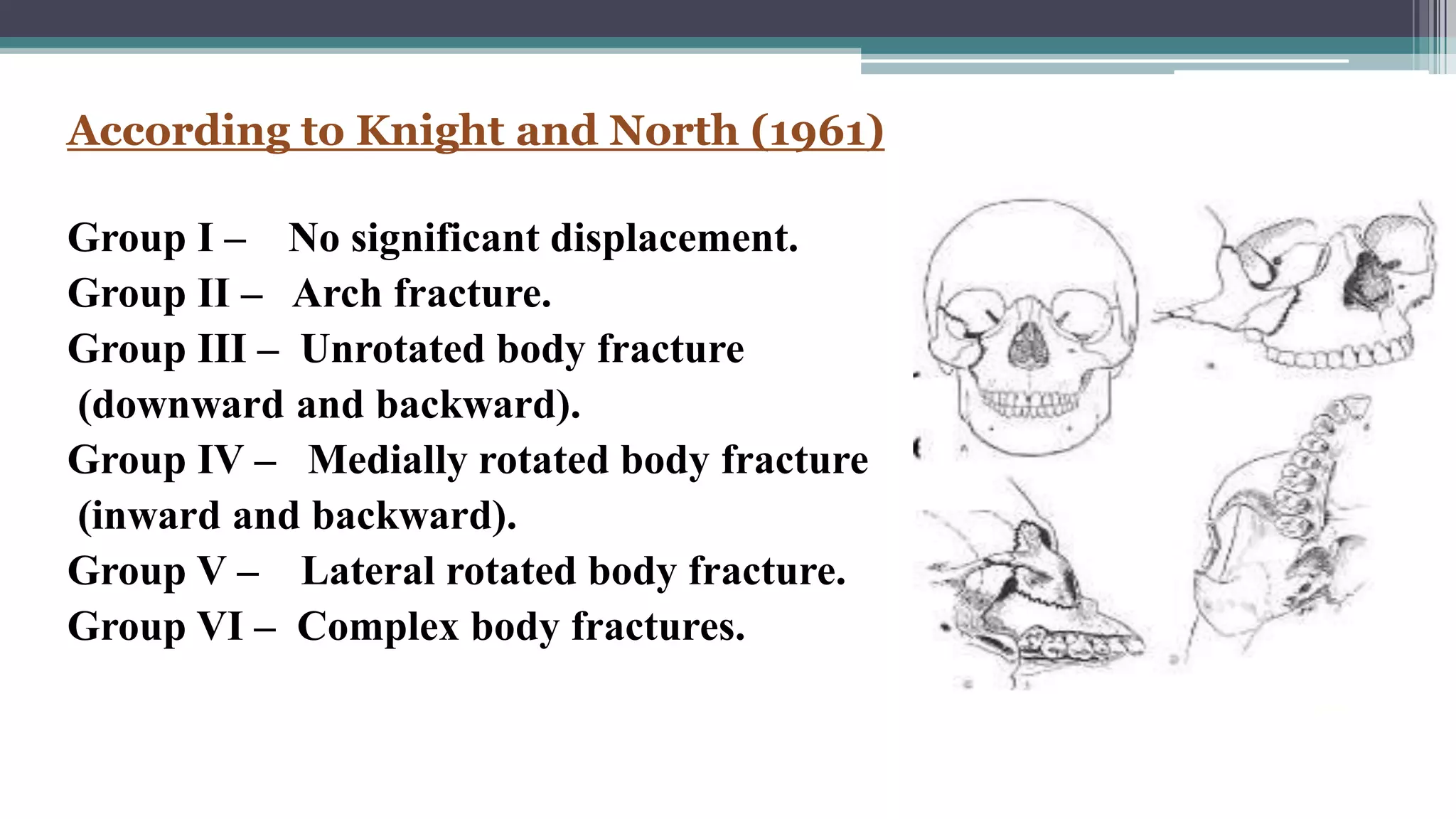
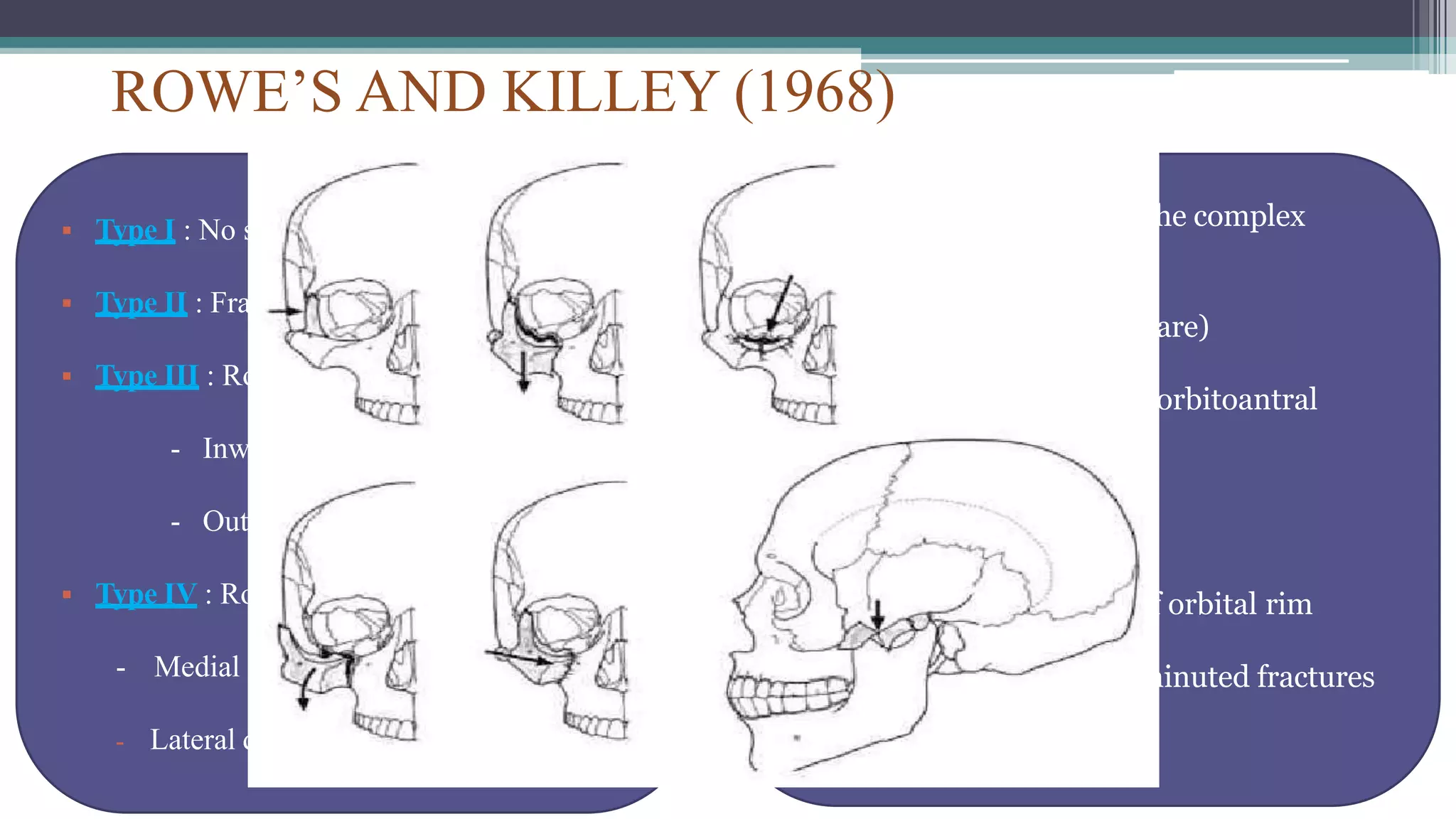
2) Common classification systems include the Knight and North system that categorizes fractures based on displacement patterns. Treatment depends on factors like displacement and stability.
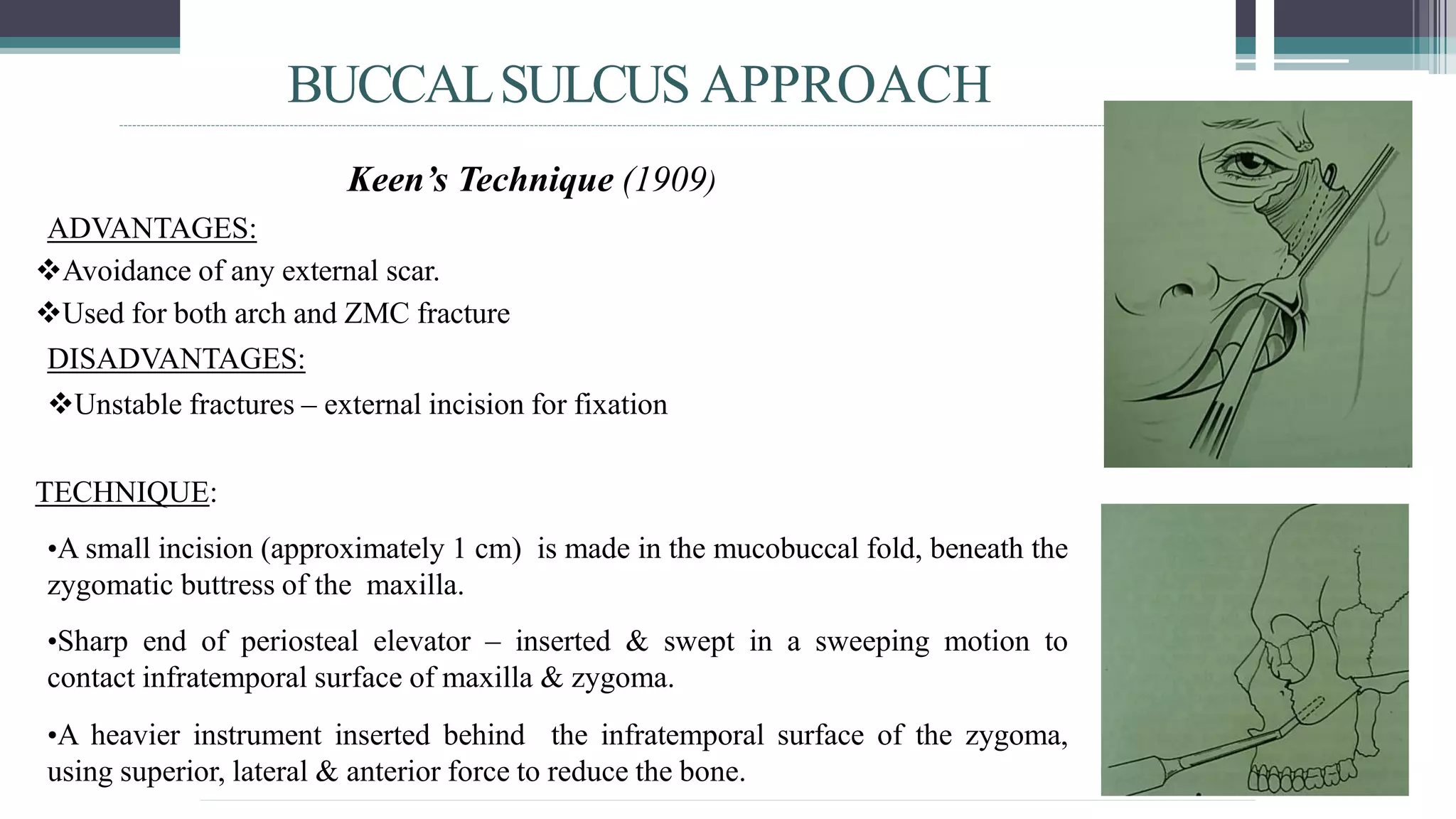
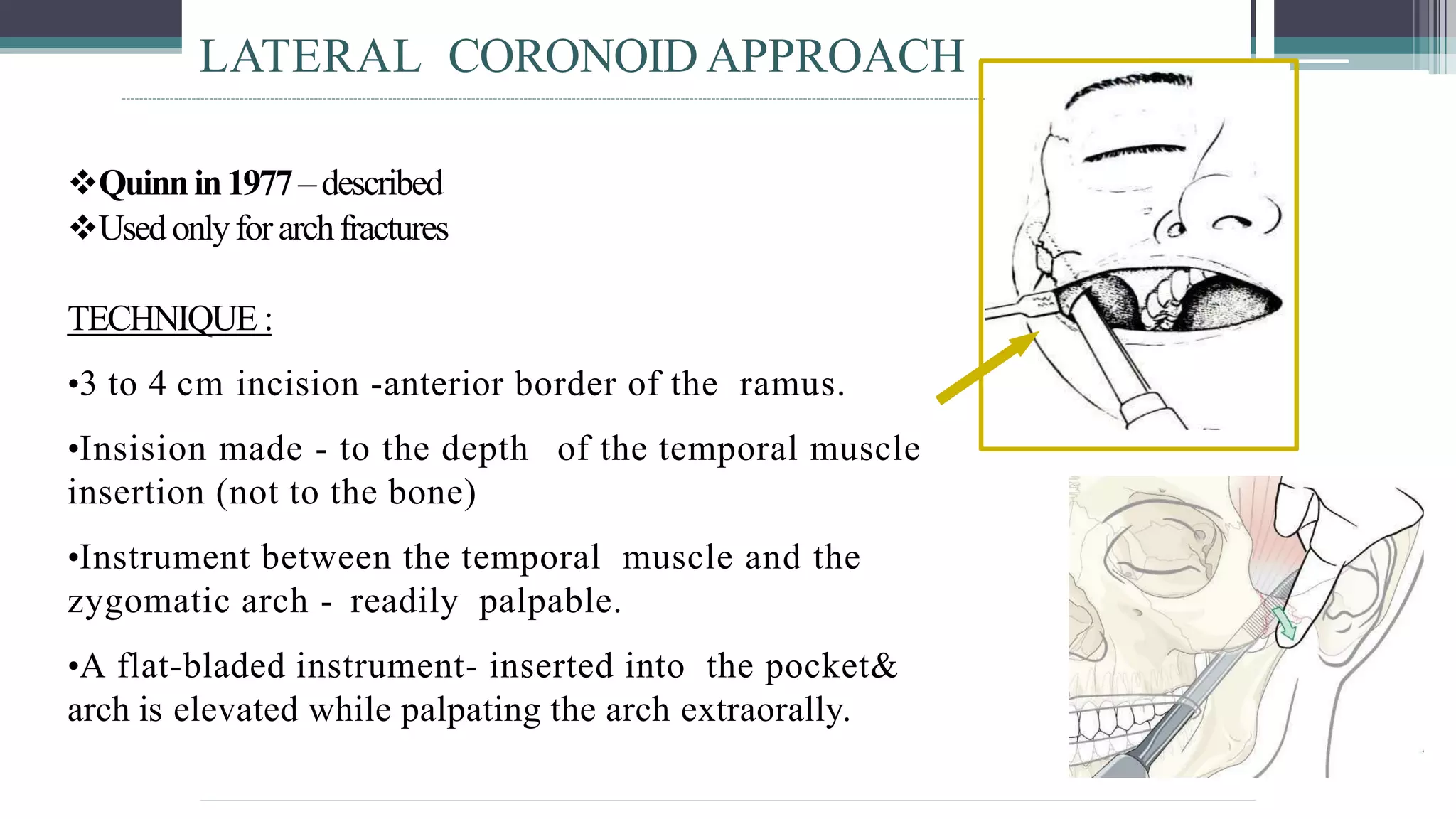
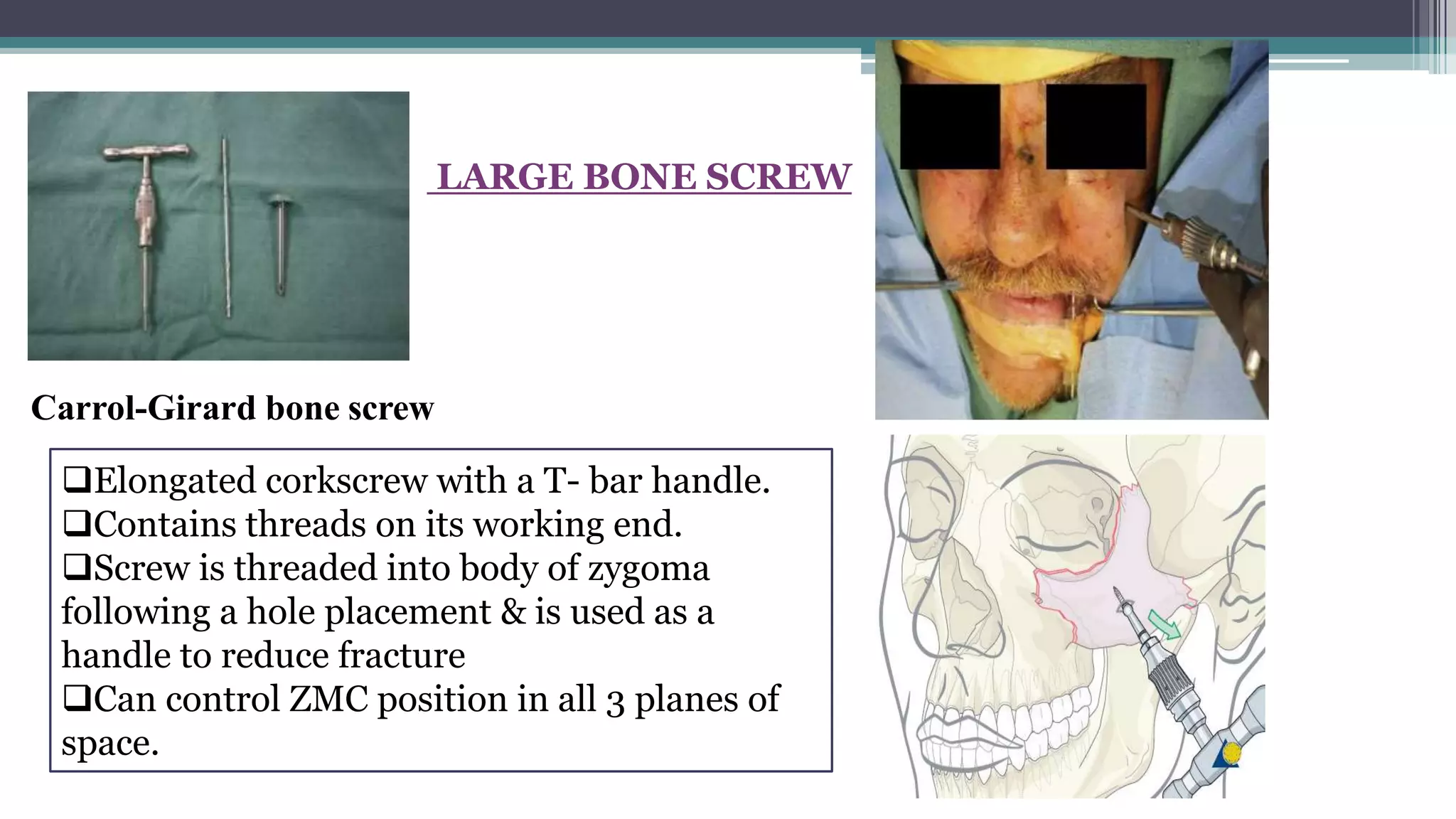
3) Approaches to treatment include no treatment for non-displaced fractures, indirect reduction using techniques like the temporal or buccal sulcus approaches, and direct open reduction using approaches like the coronal or maxillary vestibular approaches with fixation if needed.