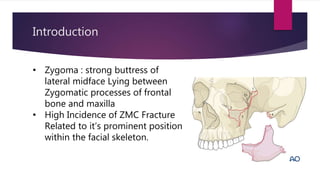
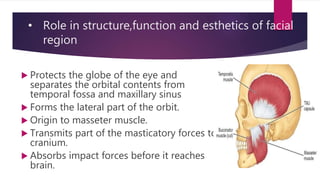
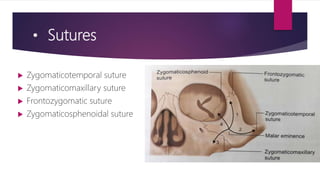
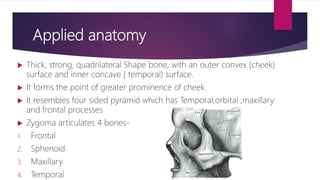
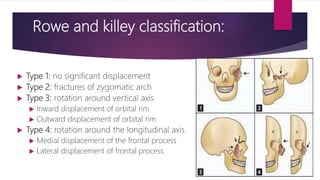
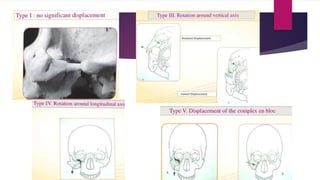
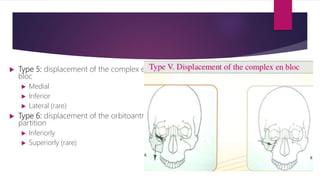
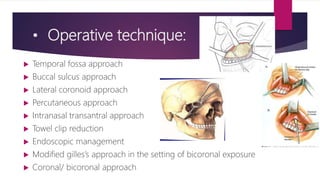
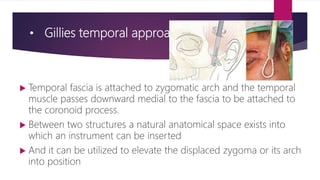
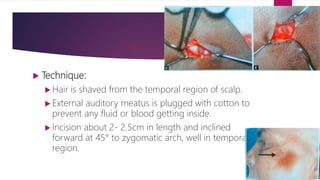
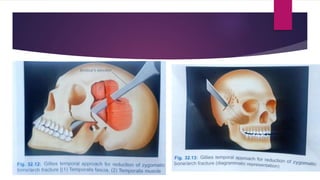
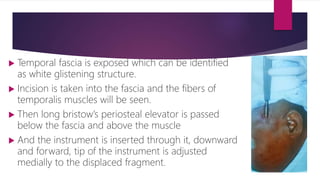
The document discusses zygomatic bone fractures, highlighting their anatomy, classification, signs, symptoms, and treatment options. It describes the importance of the zygoma in facial aesthetics and function, and outlines various types of fractures along with their management techniques. Different surgical approaches for treatment, including operative techniques, are also detailed.