1) Fractures of the zygoma are commonly caused by road traffic accidents and assaults, with the left side more frequently involved than the right.
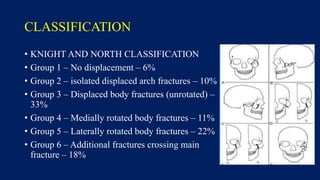
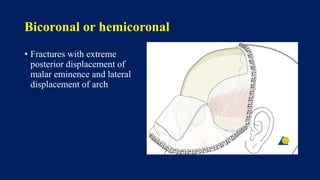
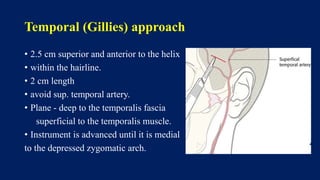
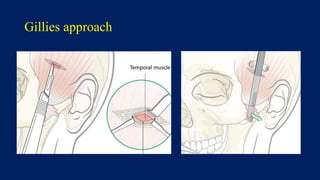
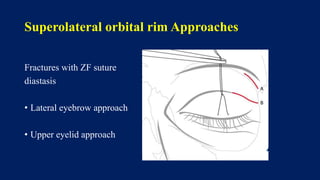
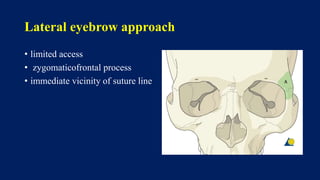
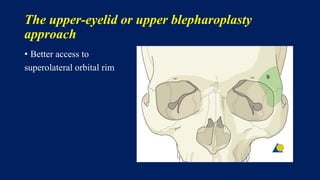
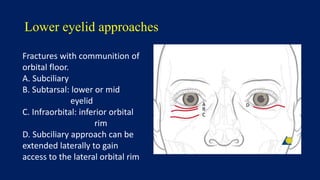
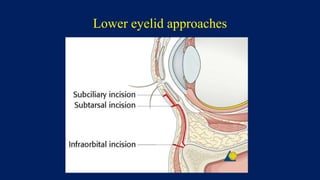
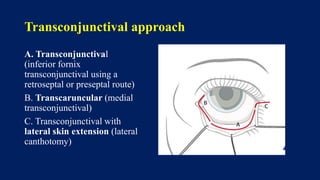
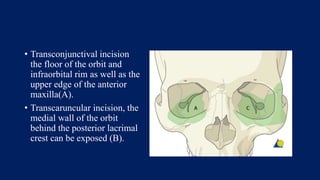
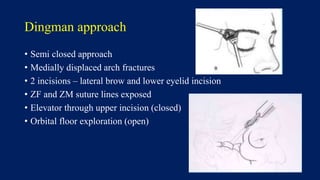
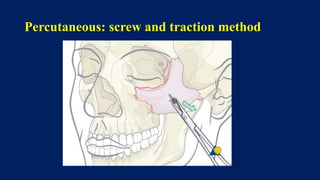
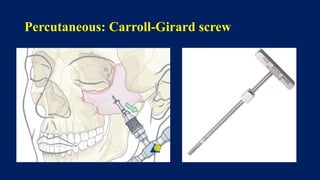
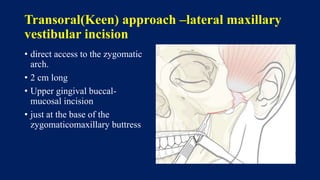
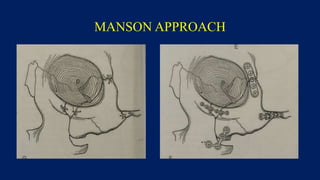
2) Classification systems categorize fractures based on the location and degree of displacement. Surgical approaches are determined by the fracture pattern and may involve extraoral or intraoral incisions.
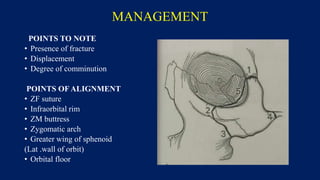
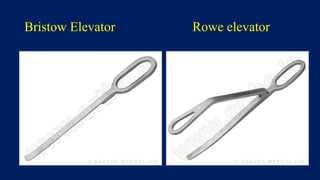
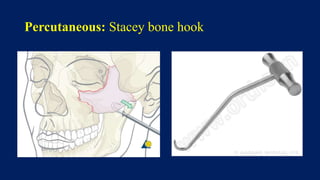
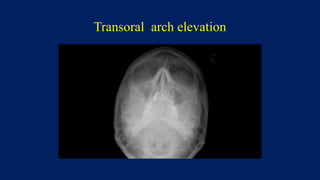
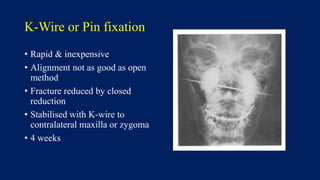
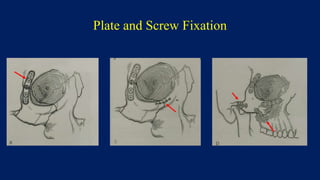
3) Treatment involves closed or open reduction and fixation using methods like K-wires, plates and screws to properly align the zygomatic arch, frontal bone sutures, and orbital rim/floor. Complications can include sinusitis, malunion, diplopia or nerve numbness if not addressed correctly.