The details on this page help your documents to be easily found.pptx
2.
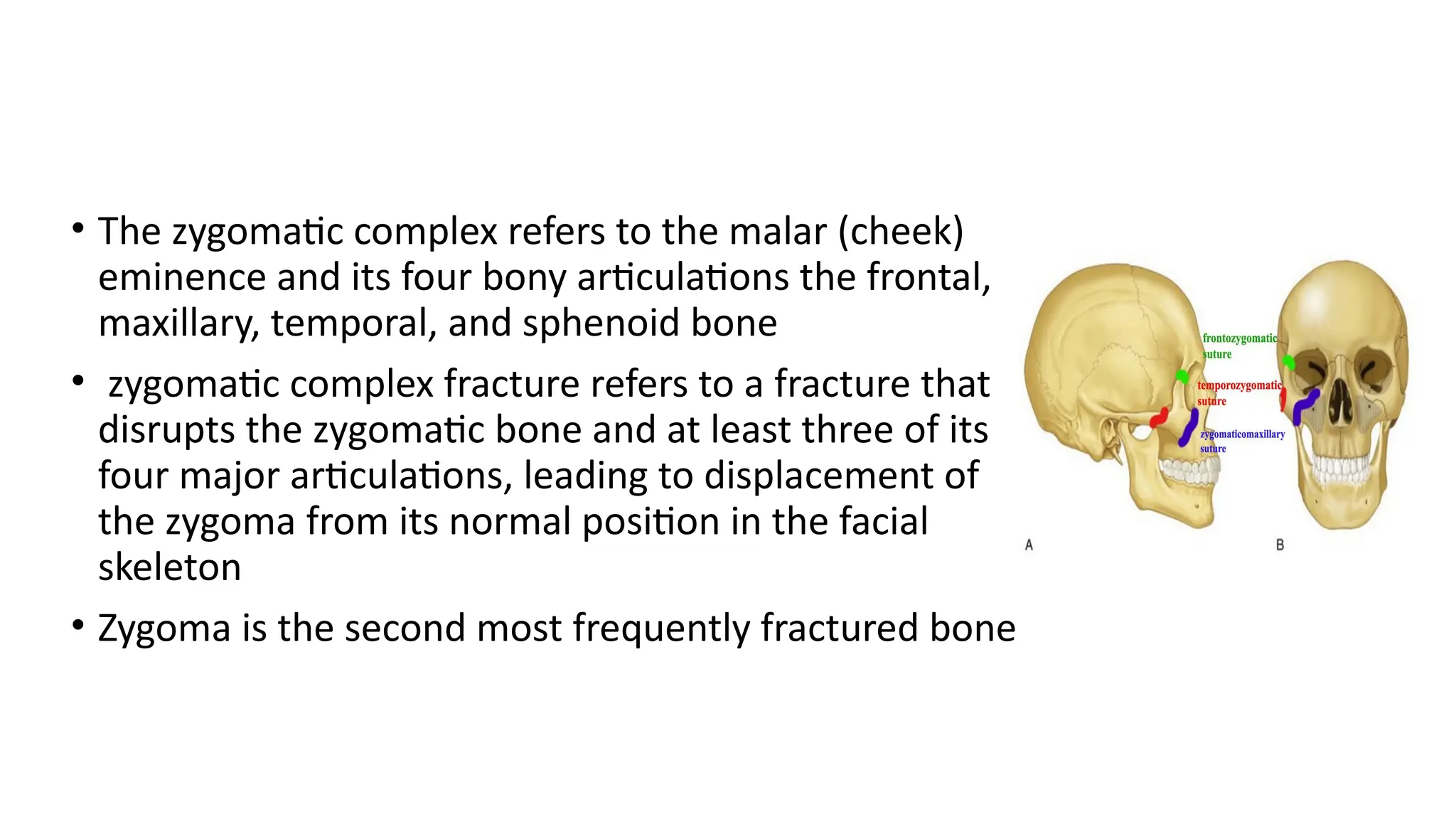
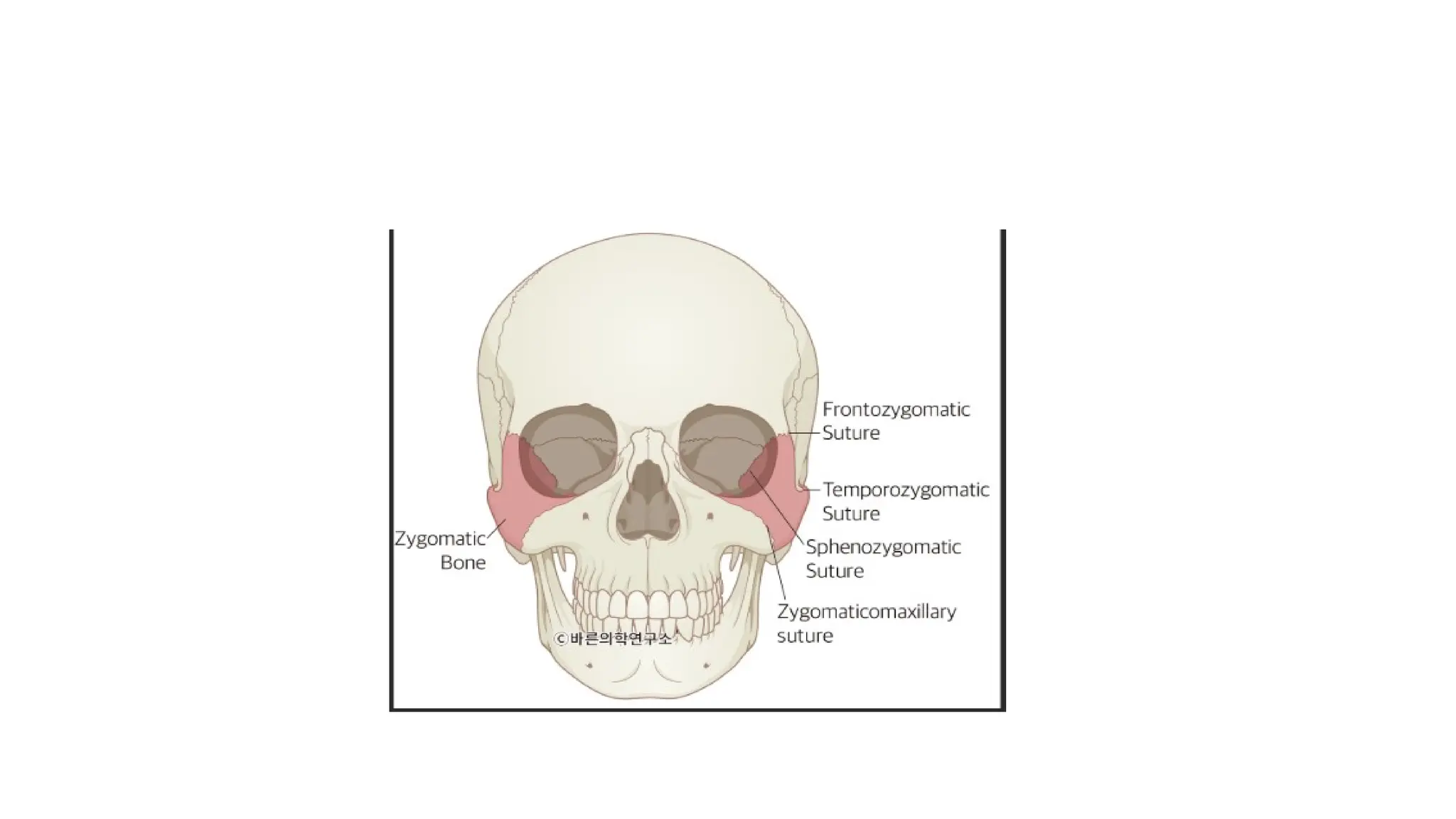
• The zygomaticcomplex refers to the malar (cheek)
eminence and its four bony articulations the frontal,
maxillary, temporal, and sphenoid bone
• zygomatic complex fracture refers to a fracture that
disrupts the zygomatic bone and at least three of its
four major articulations, leading to displacement of
the zygoma from its normal position in the facial
skeleton
• Zygoma is the second most frequently fractured bone
4.
Importance of theZygoma
• The zygomatic bone (cheekbone) gives the prominence of the cheek
and contributes to facial aesthetics.
• It forms part of the orbit, maxillary sinus wall, and zygomatic arch,
playing a vital role in:
• Protection of the eye
• Attachment for muscles of mastication and facial expression
• Maintenance of facial width and contour
• Because of its prominence and exposed position, it is prone to
trauma
5.
Common causes
1. Roadtraffic accidents (RTAs) – leading cause in most regions.
2. Assaults (fist injuries, blunt trauma).
3. Falls (especially in elderly individuals).
4. Sports injuries (contact sports)
6.
History
• The zygomaticfractures are typically diagnosed by
history and physical examination.
• The nature, force, and direction of the injuring blow
should be determined from the patient and any
witnesses
• A direct lateral blow as in an assault, often results in an
isolated zygomatic arch or an inferomedially displaced
zygomatic complex fracture
• A frontal blow usually produces a posteriorly and
inferiorly displaced fracture.
7.
clinical findings inzygomatic complex fracture
1.Swelling of cheek
2.Flattening of cheek
3.Anaesthesia of cheek, temple, upper teeth and gingiva
4. Periorbital haematoma
5.Sub-conjunctival haemorrhage
6. Tenderness over orbital rim and frontozygomatic suture
7. Step deformity of infraorbital margin
8. Palpable separation at frontozygomatic suture
9. Ecchymosis and tenderness intra-orally over zygomatic buttress
10.
Limitation of ocular movement
11.Diplopia
12.
Trismus When the arch is medially displaced.
9.
• . Eva]uationof the eye includes documentation of visual acuity,
pupillary response to light, fundoscopic examination, ocular
movement, and globe position. Limitation of motion of the
extraocular muscles, diplopia, and enophthalmos may be noted if
significant fractures of the orbital floor or medial or lateral walls are
present. Lack of pupillary response and ptosis are present if crania]
nerve III has been injured. ]nju ries to the optic nerve, hyphema,
injury to the globe, retro orbital hemorrhage, retinal detachment, and
disruption of the lacrimal ducts may also be present
10.
Radiographic Evaluation
• CT-scanis the gold standard for radiographic evaluation of zygomatic
fractures.
• Coronal views are helpful in the evaluation of orbital floor
fractures ,Soft tissue windows, in the coronal plane, are useful to
evaluate the extraocular muscles and to evaluate for herniation of
orbital tissues into the maxillary sinus
11.
Plain Radiographs
• Waters'View
Thesingle best radiograph for evaluation of zygomatic complex
fractures is Waters' view. It is a posteroanterior projection with the
head positioned at a 27-degree angle to the vertical and the chin
resting on the cassette.
12.
Caldwell's View
is aposteroanterior projection with the face at a IS-degree angle to the
cassette. This study is helpful in the evaluation of rotation (around a
horizontal axis)
13.
• Submentovertex View
Thesubmentovertex (jug-handle) view is directed from the
submandibular region to the vertex of the skull. It is helpful in the
evaluation of the zygomatic arch and malar projection
14.
• Classification: Knight& North
• The Knight and North classification (1961) categorizes zygomatic fractures by
displacement pattern into six groups :
• • Group I: No significant displacement (undisplaced)
• • Group II: Isolated zygomatic arch fracture
• • Group III: Lateral rotation of the zygoma
• • Group IV: Medial rotation of the zygoma
• • Group V: Depression (posterior displacement) of the zygoma
• • Group VI: Comminuted fracture of the zygoma
15.
• Classification: Rowe& Killey
• The Rowe and Killey system (1968) focuses on rotational deformity and post-
reduction stability . It defines seven types:
• • Type 1: Non-displaced
• • Type 2: Zygomatic arch only (no lateral wall/orbital rim involvement)
• • Type 3: Rotation about the vertical axis (A: medial rotation, B: lateral
rotation)
• • Type 4: Rotation about the longitudinal (horizontal) axis (A: medial, B:
lateral)
• • Type 5: Simple displacement without major rotation (A: medial, B: lateral,
C: posterior, D: inferior)
• • Type 6: Isolated infraorbital rim fracture (no tetrapod involvement)
• • Type 7: Complex (e.g. comminuted tetrapod) .
• Rowe–Killey classification is helpful in predicting reduction stability, as
rotational injuries (Types 3–4) may be less stable after closed reduction
16.
• Classification: Zingg
•The Zingg classification (1992) divides ZMC fractures into three types :
• • Type A (Partial/Isolated): Involves only one ZMC component (A1: arch, A2: lateral wall, A3:
infraorbital rim)
• Type B (Complete Tetrapod): All four articulations are fractured, but the zygomatic body remains
in large pieces (no comminution) .
• • Type C (Comminuted Tetrapod): All four articulations are disrupted and the zygomatic bone
itself is comminuted (multiple fragments) .
• Type A fractures are relatively uncommon; Types B and C account for the majority of ZMC injuries.
This scheme is widely used in research, as it neatly categorizes injuries by severity and need for
surgery
17.
• 1-Existing LacerationsThe use of existing lacerations should be
considered in facial fractures where soft tissue lacerations would
provide direct access to the fracture site. If necessary, existing
lacerations can be extended to attain enough access to the fracture.
However, it is advisable to place the additional incisions along the
relaxed skin tension lines (RSTLs).
18.
Treatment
• Treatment ofzygomatic fractures must be based on a complete
preoperative evaluation.
• Management of zygomatic complex and zygomatic arch fractures
depends on the degree of displacement and the resultant esthetic
and functional deficits.
19.
Zygomatic Arch Fractures
•Nondisplaced and minimally displaced zygomatic arch fractures may require no surgical
correction.
• The standard Treatment for treatment of zygomatic arch fractures, first described by Gillies, can
also be used to reduce zygomatic complex fractures.
• A temporal incision (2 cm in length) is made behind the hairline. The dissection continues through
the subcutaneous and superficial temporal fascia down to the glistening white deep temporal
fascia.The temporal fascia is incised horizontally to expose the temporalis muscle.
• Rowe zygomatic elevator, is inserted deep to the fascia, underneath the temporal surface of the
zygoma. The elevator must pass between the deep temporal fascia and temporalismuscle or it
will be lateral to the arch.The bone should be elevated in an outward and forward direction, with
care taken not to put force on the temporal bone. The arch should be palpated at all times as a
guide to proper reduction. The wound is closed in layers.
• Open reduction with internal fixation is seldom necessary for treatment of isolated zygomatic
arch fractures.
20.
Surgical Approach tothe Zygomaticomaxillary
Buttress.
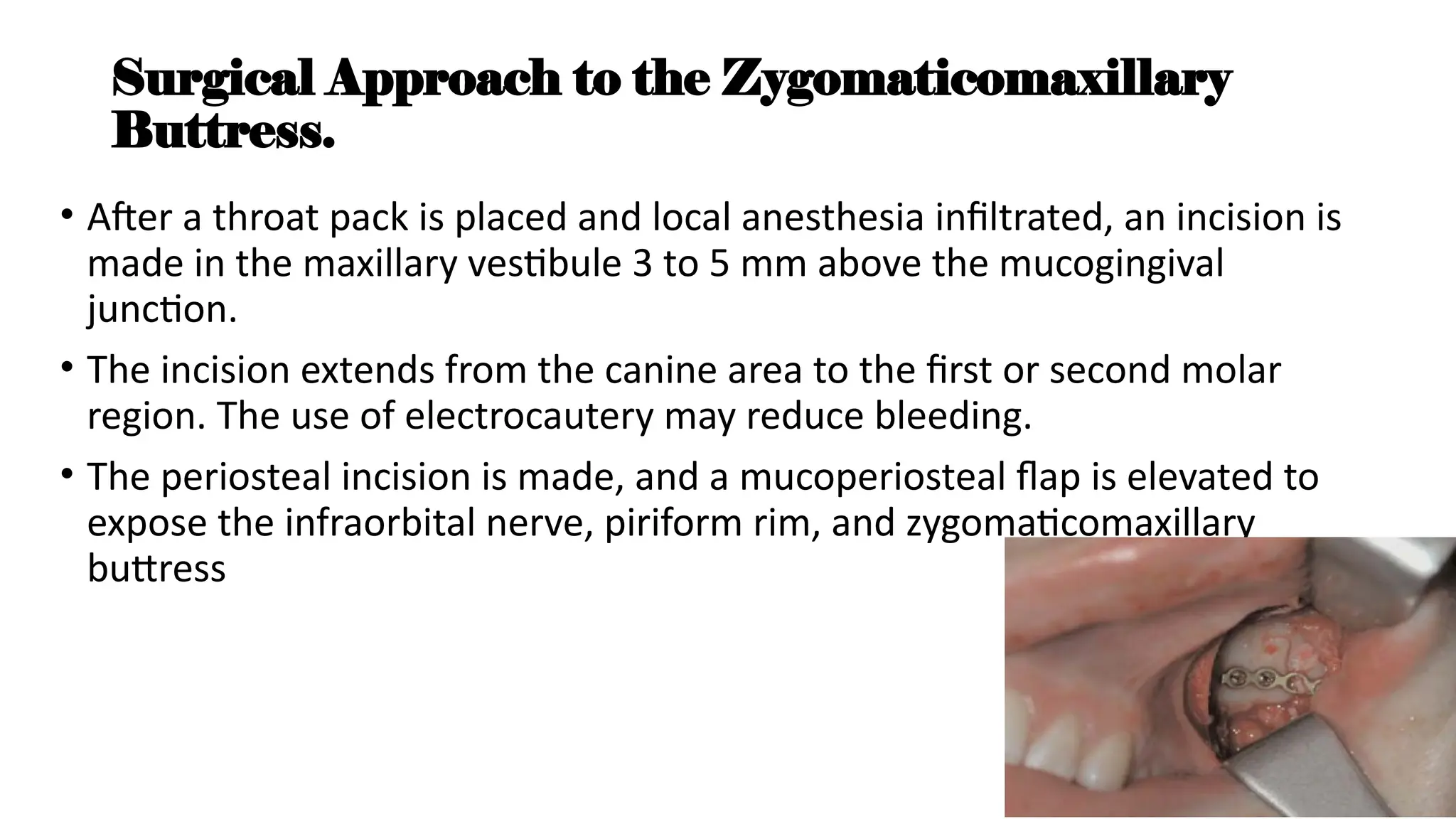
• After a throat pack is placed and local anesthesia infiltrated, an incision is
made in the maxillary vestibule 3 to 5 mm above the mucogingival
junction.
• The incision extends from the canine area to the first or second molar
region. The use of electrocautery may reduce bleeding.
• The periosteal incision is made, and a mucoperiosteal flap is elevated to
expose the infraorbital nerve, piriform rim, and zygomaticomaxillary
buttress
21.
Surgical Approach tothe Zygomaticofrontal
Buttress.
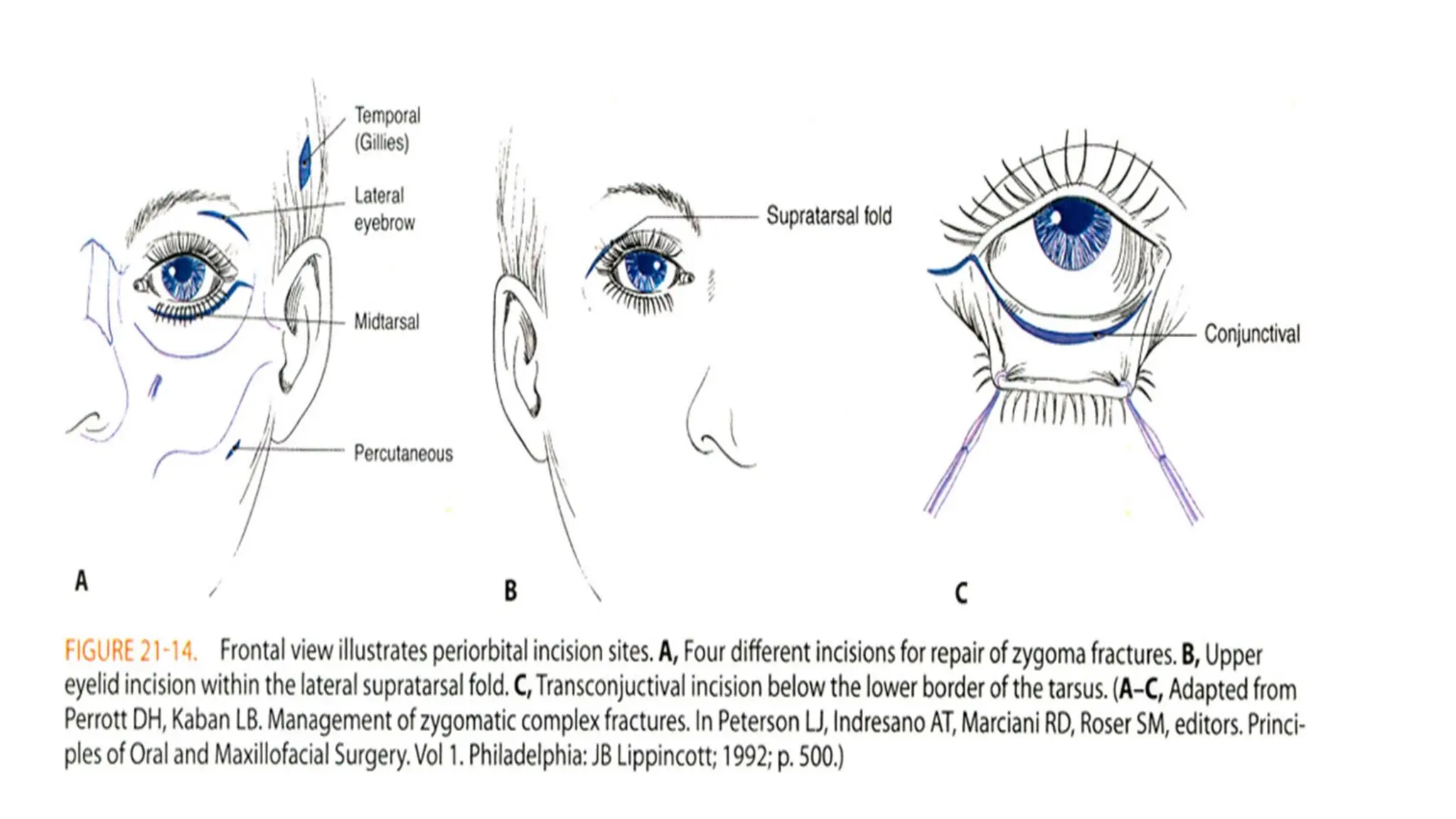
• Access and exposure for open reduction of the zygomaticofrontal buttress can be
achieved through a supratarsal fold or lateral eyebrow incision. If present, a preexisting
laceration may be used for exposure of this region.
• The supratarsal fold incision for approach to the lateral orbit.
• The incision is placed in a skinfold parallel to the superior palpebral sulcus above the
tarsal plate. It is placed approximately 10 to 14 mm above the margin of the upper eyelid.
• Blunt dissection parallel to the orbicularis oculi muscle fibers separates them and exposes
the lateral orbital rim.
• A vertical periosteal incision is made, and subperiosteal dissection will expose the
fracture. The incision provides access to the frontozygomatic suture and results in a less
noticeable scar.
• A lateral brow incision is performed by first palpating the frontozygomatic suture.
23.
• For morecomplex injuries that may require exposure of all three
anterior buttresses, the zygoma ticofrontal fracture may be first
stabilized temporarily with an interosseous wire.28,31This is followed
by fixation of the zygomaticomaxillary fracture and the infraorbital
rim if indi cated. The temporary wire at the zygomaticofrontal fracture
24.
Internal Fixation
• InternalFixation Historically, many methods have been used for stabilization of
zygomatic complex fractures. These have included antral packing, percutaneous
wire fixation, and wire osteosynthesis. It is now accepted that miniplate or
microplate fixation provides the best results and minimal complications.
• Controversy exists regarding the best location for internal fixation and the
number and type of plates required.
• Multiple studies have tried to characterize the forces placed on the zygomatic
complex and the amount of fixation required to achieve“stability.
• These forces include the masseter and temporalis muscles and fascia and soft
tissue contracture, which cause rotational movements in multipleaxes around
the zygomatic buttresses
25.
Internal Fixation ofthe Zygomaticomaxillary
Buttress
• The zygomaticomaxillary buttress provides an ideal location for
internal fixation for middle- and high energy fractures.
• Anatomic reduction of this fracture assists in restoring malar
projection, but is difficult if the buttress is comminuted. The overlying
soft tissue is thick, and plate palpability is not a concern. Therefore,
this fracture should be stabilized with 1.5 or 2.0 plates
27.
Sequence of InternalFixation
• For middle-energy injuries with exposure of all three anterior
buttresses,The zygomaticofrontal fracture may be stabilized temporarily
with an interosseous wire.
• This is followed by fixation of the zygomaticomaxillary fracture and the
infraorbital rim.
• The temporary wire at the zygomaticofrontal fracture is replaced with a
plate.
• The orbital floor is reconstructed after the zygoma has been restored to
its correct three-dimensional position.
• In high-energy fractures, the zygomatic arch should be reconstructed first.
28.
Internal Fixation ofthe Zygomaticofrontal
Buttress.
• The zygomaticofrontal buttress contains excellent bone for fixation
and can accommodate a 2.0 plate.
• The reduction and fixation of this fracture will reestablish the vertical
height of the zygomatic complex. However, because of its narrow
interface, this buttress may not be as helpful in evaluating reduction
of a rotated fracture. The thickness of the soft tissue overlying this
region is variable. In some instances it may be quite thin and a large
plate may be palpable. If stable fixation can be achieved at other sites,
a smaller platemay be used.
29.
Internal Fixation ofthe Infraorbital Rim
• Unlike the zygomaticofrontal buttress, the infraorbital rim has poor
quality bone for internal fixation.Additionally, the lower eyelid skin is
quite thin, and large plates are easily palpable.
• Despite these concerns, fixation of this site is required to define the
orbital volume and facial width.
• The infraorbital rim is typically displaced posteriorly and inferiorly.The
fracture should be mobilized anteriorly and superiorly and stabilized.
Typically a 1.0 or 1.5 microplate is used to stabilize the infraorbital
rim.
30.
Internal Fixation ofthe Zygomatic Arch
• Internal fixation of the zygomatic arch is required for high-energy
fractures that demonstrate comminution and lateral displacement.
• Restoration of this sagittal buttress assists in restoring facial
projection and facial width.
• width.When exposed, the zygomatic arch is often reduced and
stabilized first in the sequence of repair ofhigh-energy injuries.
• Caution must be used in restoring a “straight” arch and not a curved”
arch, which will decrease facial projection. This fracture typically
requires a large plate to resist deformational forces
31.
Postoperative Care
• Zygomaticcomplex fractures violate the maxillary sinus. For this reason,
periorperative antibiotics and decongestants are recommended
particularly if a transoral approach is used or an implant placed.
• Ampicillin, amoxicillin, clindamycin, or cephalosporin may be
used,decongestant such as pseudoephedrine may also be indicated.
Incisions are observed carefully for signs of infection, and the eye is
examined to document visual acuity and to rule out complications such
as corneal abrasion.
• Postoperative imaging should be obtained to document reduction of the
fracture and orbital reconstruction.
Infraorbital Paresthesia
1. Theincidence of sensory alterations of the infraorbital nerve after
zygomatic trauma ranges from 18% to 83%.
2. nondisplaced midfacial frac tures had post-traumatic infraorbital nerve
impairment with a mean recovery time of 4 weeks.
3. In displaced midfacial fractures, (90%) had altered sensation within the
infraorbital nerve distribution with a mean recovery time of 13 weeks.
4. Incomplete recovery was frequently associated with intraoperative
evidence of direct nerve injury.
5. The authors support early open reduction and internal fixa tion to
improve recovery of post-traumatic nerve dysfunction.
34.
Malunion and Asymmetry
1.Inadequate reduction or stabilization of zygomatic fractures may result
in malunion or asymmetry,Poor malar projection is the result of
uncorrected inferior and posterior rotation of the zygoma,Increased
facial width Malunion that is recognized up to 6 weeks after injury may
be corrected using routine zygomatic reduction techniques.
2. Correction of mild late deformities includes autogenous onlay grafts or
placement of alloplastic implants such as porous
35.
Enophthalmos
• Enophthalmos isone of the most troubling complications after
orbitozygomatic fractures. An increase in orbital vol ume is the most
common etiology
• Clinically, poor alignment of the orbital rim may significantly increase the
orbital vol ume and result in enophthalmos.
• Orbital floor blow-out fracture also may result in enophthalmos by
increasing the orbital volume
• Late repair of enophthalmos is technically challenging. Wide access with
osteotomy of the zygoma, repositioning, and grafting is usually required.
Redraping of the periorbital soft tissue including a canthopexy may be
required
36.
Diplopia
• Diplopia isa common sequela of midfacial fractures.
• The principal causes of diplopia include edema and hematoma, entrapment of
the extraocular muscles and orbital tissue, and injury to cranial nerve III, IV, or
VI, post-traumatic fibrosis of the extraocular muscles in response to injury
• Axial and coronal CT scans and ophthalmologic consultation are recommended
to assist in evaluation.33.92 Diplopia related to edema, hematoma, or
neurogenic causes may resolve without intervention.
• Diplopia resulting from entrapment requires exploration and reduction of
herniated orbital tissue Persistent
• diplopia that does not resolve may require treatment by an ophthalmologist.
The condition may respond to exercise or surgery.
37.
Traumatic Hyphema
• Traumato the eye may result in bleeding into the anter ior chamber-the
area between the clear cornea and the colored iris Ophthalmology
consultation is recommended. Goals of treatment include prevention of
rebleeding, which may occur in 5% to 30% of patients, and maintenance
of normal ocular tension
• Management of hyphema consists of supportive therapy including
elevation of the head of the bed and patching of the injured eye. Medical
management includes topical cycloplegics, corticosteroids, and beta
blockers
• Rarely, surgical intervention by the ophthalmologist is required. Repair of
fractures may be delayed.
38.
• Retrobulbar hemorrhageis a rare but severe compli cation that may be the
result of either the initial injury or the operative correction. Disruption of
the retinal circulation may lead to irreversible ischemia and permanent
blindness.
• reported a 0.03% incidence of postoperative retrobulbar hemorrhage with
visual loss. An emergent ophthalmologic consultation is necessary;
however, decompression with lateral canthotomy and cantholysis should
not be delayed
40.
• Patients withzygomatic fractures commonly present acutely with a
complaint of trismus.
• The most likely cause is impingement of the zygomatic body on the
coronoid process of the mandible.
• If the zygoma is improperly reduced, zygomatic osteotomy and
repositioning may be necessary to restore unrestricted motion of the
mandible.

![• . Eva]uation of the eye includes documentation of visual acuity,
pupillary response to light, fundoscopic examination, ocular
movement, and globe position. Limitation of motion of the
extraocular muscles, diplopia, and enophthalmos may be noted if
significant fractures of the orbital floor or medial or lateral walls are
present. Lack of pupillary response and ptosis are present if crania]
nerve III has been injured. ]nju ries to the optic nerve, hyphema,
injury to the globe, retro orbital hemorrhage, retinal detachment, and
disruption of the lacrimal ducts may also be present](https://image.slidesharecdn.com/zmcfracture-251021111424-cd848481/75/The-details-on-this-page-help-your-documents-to-be-easily-found-pptx-9-2048.jpg)