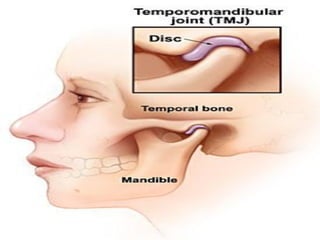



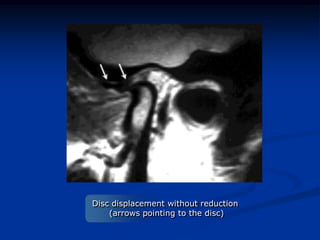

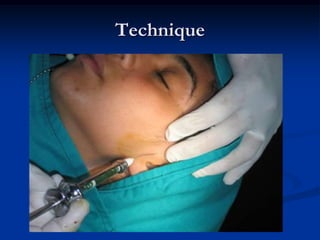






This document provides an overview of internal derangements of the temporomandibular joint (TMJ). It defines internal derangement as an abnormal relationship between the articular disc and condyle. The most common type is anterior disc displacement, which can be with or without reduction. Causes include trauma, functional overloading, joint laxity, and muscle spasms. Symptoms vary depending on the type but may include clicking, limited opening, and pain. Diagnosis involves clinical exams and MRI imaging. Treatment ranges from splint therapy to arthrocentesis or arthroscopy for lavage and relief of adhesions. Arthrocentesis is shown to improve opening and reduce pain by removing inflammatory factors from the



























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







