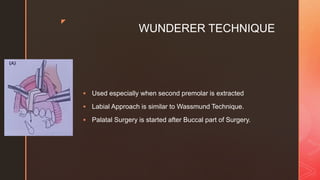
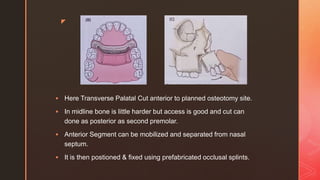
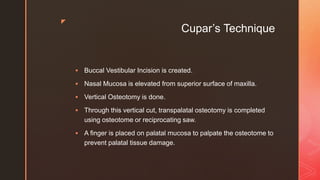
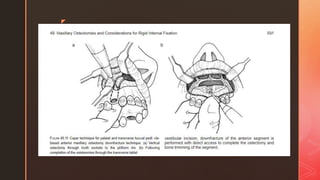
This document discusses anterior segmental maxillary osteotomy techniques. It provides a brief history, noting the first osteotomy was performed in 1921 using a wedge resection. Current indications include correcting protruding maxillary anterior teeth and anterior open bites. Techniques described include the Wassmund, Wunderer, and Cupar's approaches. The Wassmund technique involves vertical incisions between the canine and premolar with palatal osteotomies. Fixation methods after repositioning the anterior segment include occlusal splints, wiring, or plates. Potential complications are also outlined.