Introduction
• Fractures ofthe zygoma are relatively common
• Constitute 60 – 70% of all midfacial fractures
• The zygoma represents a prominent position in the facial skeleton as a
whole
• The zygomatic bone is intimately associated with the maxilla, frontal
and temporal bones
• They are usually involved when a zygomatic bone fracture occurs
hence the term zygomatic complex fractures
• Zygomatic bone usually fractures in the region of the frontozygomatic,
the zygomaticotemporal and zygomaticomaxillary sutures
• Unusual for the zygomatic bone itself to be fractured, but occasionally
may be split across and when there has been extreme fracture violence
the bone may even be comminuted.
4.
Current Concept 1
•Zygomatic Complex Fracture is not a tripod fracture rather
it is a tetrapod fracture
• It articulates with the frontal, maxillary, and temporal bones
and the orbital extension of the zygoma has a broad
abutment with the greater wing of the sphenoid thus making
it a tetrapod
• This surface of the zygoma constitutes most of the lateral
orbital wall and also forms part of the orbital floor lateral to
the infra orbital groove
5.
• Thus adisplaced zygomatic fracture is also an orbital floor
fracture
• Failure to accurately position the lateral orbital complex as well
as insufficient repair of the orbital floor can be a major factor
in the development of post traumatic visual disturbances
• Inaccurate three dimensional restoration of the original
configuration of the malar complex will eventually result in
enlargement of the orbital cavity
• Any minor displacement of the malar prominence leads to
unfavourable esthetic results
7.
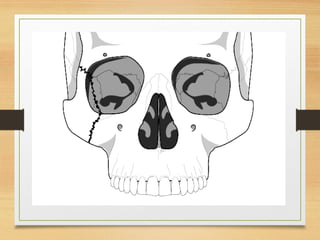
Anatomical considerations
• Theintegrity of the zygoma is well established as critical in
the maintenance of facial width and maintenance of the
cheek
• By making the anterior lateral floor, it is a major contributor
to the orbit
• Attached to the zygoma anteriorly are the zygomaticus major
and minor muscles as well as the orbicularis oculi muscles.
• Laterally the masseter muscle from below attaches to the
zygomatic arch and produces displacing forces on the zygoma
8.
Current Concept 2– Presence of
Structural buttresses
• Depiction of the facial anatomy in terms of the
structural pillars and buttresses
• This concept allows consideration of an approach
for reduction of midfacial fractures and ultimately
the production of a stable reconstruction
• Midface is made up of sinuses that are supported
fully and fortified by vertical and horizontal
buttresses of bone
9.
Three main buttresses
•The medial or nasomaxillary buttresss which reaches the
frontal cranial attachment from the anterior maxillary
alveolus
• The pterygomaxillary or posterior buttress which connects
posterioirly the maxilla to the sphenoid bone
• The lateral or zygomaticomaxillary buttress which connects
the lateral maxillary alveolus to the zygomatic process of
temporal bone
• These buttresses give the zygoma an intrinsic strength such
that blows to the cheek usually results in fractures of the
zygomatic complex at the suture lines
10.
• Fracture linesusually run through the infraorbital rim
involve the posterolateral orbit and extend to the inferior
orbital fissre
• The fracture line then continues to the zygomatico sphenoid
suture area and on to the frontozygomatic suture line
• All zygomatic complex fractures involve the orbit making
visual complications a frequent occurrence
11.
• The sphenozygomaticjunction is an important landmark for
reduction of zygomatic fractures
• The alignment of the zygoma with the greater wing of
sphenoid in the lateral orbit is critical for determining
adequate reduction of zygomatic fractures
• Reducing the three points that make up the buttresses also
helps to ensure proper alignment of the zygoma and proper
reduction of other facial fractures present
12.
• The graduatedapproach helps to preserve facial height
and width
• The branches of the fifth and seventh cranial nerves live
within the bounds of midfacial region
• The temporal and zygomatic branches of the facial
nerve and the zygomaticotemporal and the
zygomaticofacial branches of the fifth nerve must be
carefully dissected to avoid complications of paresis and
paresthesias
13.
Classifications
• Different typesof classification have been proposed
• Most of the classification are descriptive and do not take into
consideration the three dimensional nature of these fractures
and their surgical implications
• An attempt to use the axial CT images showed the shortcoming
• Without coronal CT images the three dimensional
configuration of the fracture is not readily apparent and in high
energy traumas it is imperative to rule out concomitant anterior
skull base injuries
14.
• Fickling (1948)
•Knight and North (1961)
• Rowe and Killey (1968)
• Pozatek et al (1973)
• Manson et al (1986)
• Zigg et al classification (1992)
15.
Knight and North(1961)
• Group 1 –Undisplaced fractures
• Group 2 –Arch fractures
• Group 3- Unrotated body fractures
• Group 4- Medially rotated body fractures
• Group 5- Laterally rotated body fractures
• Group 6 – Complex fractures
16.
Manson (1986)
• Mansonand colleagues have proposed a more
modern classification system in which CT Scan is
used as a backbone
• CT provides abundant information about facial
fractures
• The bony displacement and segmentation are noticed
• This helps to appropriately address all aspects of
injury
17.
• Manson’s systemdivides fractures into low energy,
medium energy and high energy injuries
• Low energy injuries demonstrate little or no
displacement with stability provided by an
incomplete fracture
• The type of fracture is seen at the zygomatico frontal
suture
• The inherent stability does not justify a reduction
18.
• Middle energyfractures demonstrate complete
fractures at all buttresses
• Mild- moderate displacement and a wide range of
comminution
• Often an eyelid and intraoral exposure is necessary
for adequate reduction and fixation
19.
• High energyzygoma fractures frequently accompany
LeFort or panfacial fractures as a segment of these
injuries
• These fractures often extend through the glenoid fossa
• They permit extensive collateral and posterior
dislocation of the arch and malar eminence
• A coronal exposure in addition to the oral and eyelid
incisions necessary
20.
ZIGG ET AL(1992)
• Type A: Incomplete zygomatic fracture- Fracture of only the
zygomatic pillar. This may be an isolated zygomatic arch
fracture (A1), a lateral orbital wall fracture (A2) or an
infraorbital rim fracture (A3). Displacement of the malar
complex does not occur because the remaining pillars are intact
• Type B: Complete monofragment zygomatic fracture (tetrapod
fracture) All four pillars of the malar bone are fractured and
displacement may occur
• Type C: Multifragment zygomatic fracture. Same as type B but
with fragmentation, including the body of the zygoma.
21.
• Occasionally thedistinction betweeen Type A, B and
C fractures are evident on high resolution CT only.
Clinical features
• Ocularand periorbital signs
• Periorbital Eodema
• Periorbital ecchymosis
• Subconjunctival ecchymosis
• Chemosis
• Diploplia
• Enopthalmos
• Restriction of ocular movement
• Lowering of ocular level
• Tenderness at the lateral orbital rim
• Bony discontinuity at the lateral orbital
rim
• Step deformity at the lateral orbital
wall
• Tenderness at the infraorbital rim
• Bony discontinuity at the infraorbital
rim
• Step deformity at the infraorbital rim
• Nasal sign
• Epistaxis
• Neurological sign
• Paresthesia or Anaesthesia of areas
innervated by Infraorbital nerve
• Intraoral signs
• Transient Gagging of occlusion in the
molar area
• Anaesthesia of gum and teeth
• Ecchymosis in the buccal sulcus
• Tenderness on zygomatic buttress
• Bony discontinuity at the zygomatic
buttress
• Step deformity at the izygomatic
buttress
• Others
• Flattening of the cheek
• Interference with mandibular excursion
• Treatment –Indications for surgical intervention
• Functional
• Diplopia that persist for more than 7 -10
days
• Interference with mandibular excursion
• Disorganization of periorbital bones
• Aesthetics
• Flattening of the face
27.
Treatment- Aims
• Torestore the normal contour of the face both for
cosmetic reasons
• To establish the skeletal protection of the globe
• To correct diplopia
• To remove any interference with the range of
mandibular movement
Fixation
Temporary support
• WhiteheadVARNISH(antral pack)
• Foley’s catheter
Direct Fixation
• Transosseous wiring
• Bone plates
Indirect fixation
• Bone pin fixation
31.
• A 2point fixation leaves an axis of rotation for the zygoma
following an adequate reduction
• Forces such as the masseter often displace the zygoma
postoperatively
• Therefore choice to establish 3 point fixation and ultimate
stability is important
• Primary bone healing allows quicker and stronger healing of
a fracture than callous healing
• In rigid fixation bone heals by primary processes
32.
• Some biomechanicalmodels predict backward,
downward and medial rotation of zygoma with 2
point alignment
• Miniplates are superior to wires. Rigid miniplates
offer the best form of fixation
• Titanium miniplates found to be the strongest in
distraction and compression across a central gap
33.
The use ofBiodegradable
Materials
• Biodegradable materials- Polymers and copolymers
of Poly L lactic acid, Poly D Lactic acid, Polyglycolic
acid and poly dioxanone- sulphate
• A copolymer of PLLA and PGA in a ratio of
82/18% was the first commercially available for the
fixation of maxillofacial fractures (Lactosorb)
34.
The use ofappropriate incisions
• Temporal and supraorbital for lateral orbital rim
• Gingivobuccal incision for the buttress
• Transconjuctival incision for Infraorbital rim
• Subciliaryincision for Infraorbital rim
• Infraorbital for Infraorbital rim
• Coronal exposure for lateral orbital rim and the Arch
• Endoscopically assisted operations
35.
Complications
• Infraorbital nervedysfunction
• Trismus
• Persistent Diplopia
• Persistent Enopthalmos
• Infection
• Complication with plates and screws – Breakage and
migration

































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















