Download to read offline


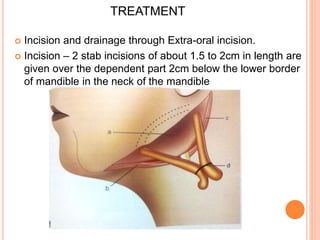
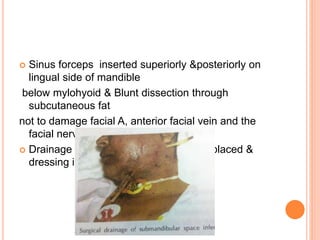

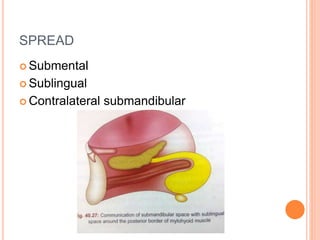
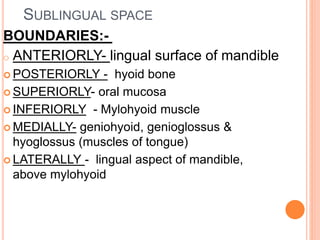
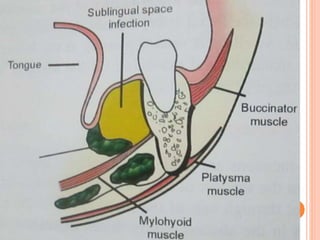
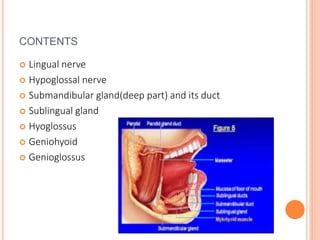
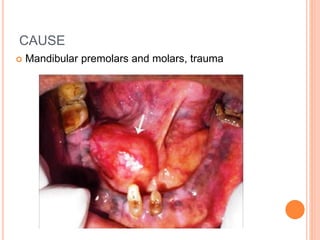
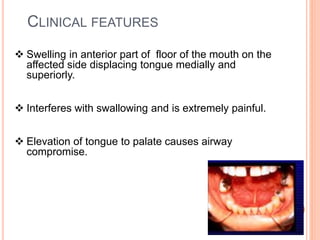
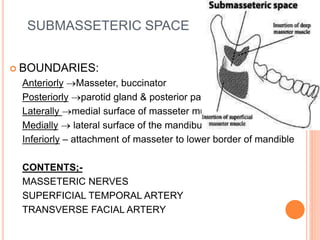
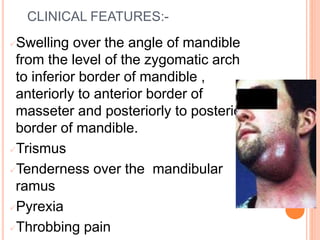
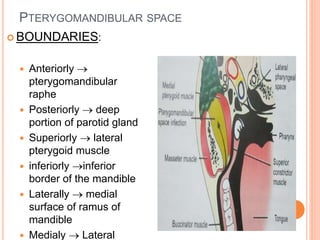
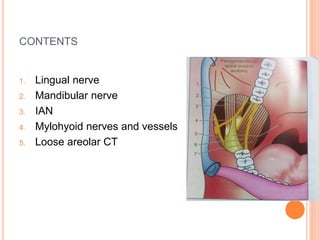


This document discusses various fascial spaces in the head and neck region that can become infected, including the mandibular, submandibular, sublingual, buccal, submasseteric, pterygomandibular, and lateral pharyngeal spaces. It describes the boundaries, contents, potential causes of infection, clinical features, and treatment approaches for infections in each of these spaces. The treatment typically involves incision and drainage of the abscess through both intraoral and extraoral incisions as needed depending on the specific involved space.























































































