Downloaded 496 times
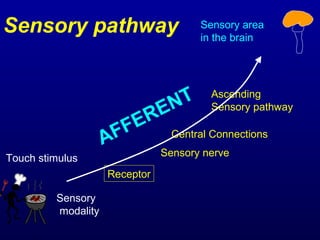

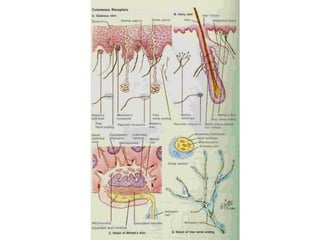
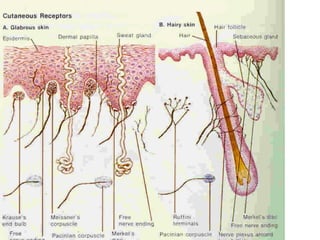
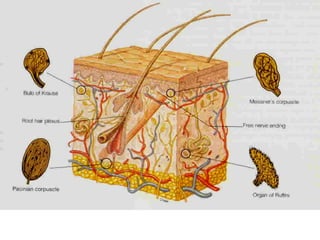
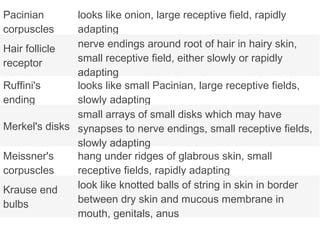
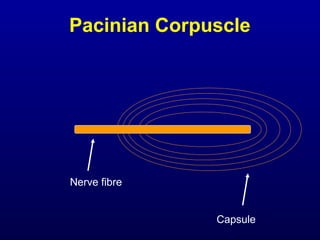
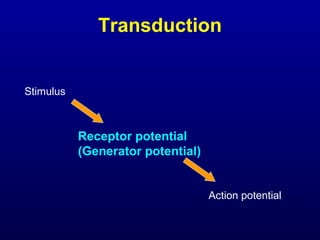
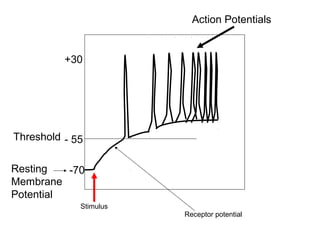
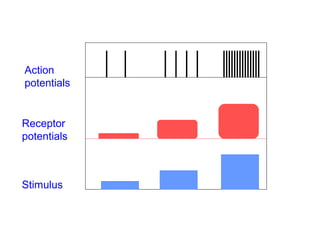
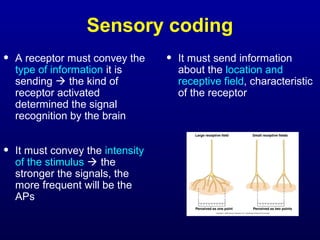
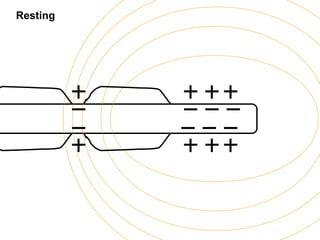
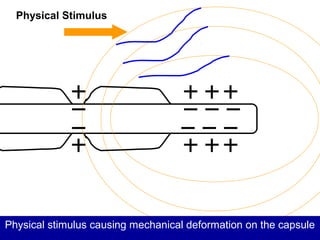
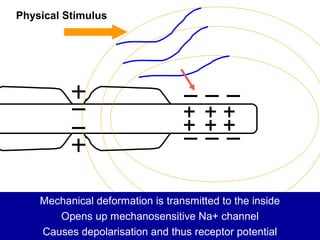
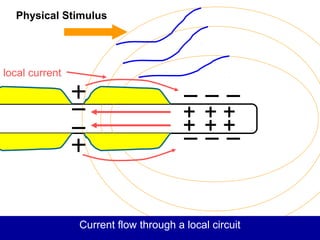
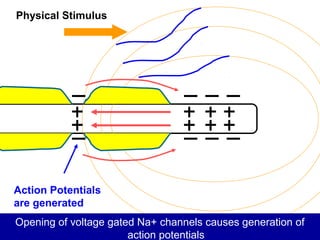
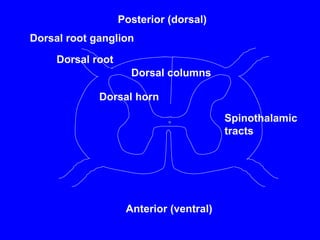
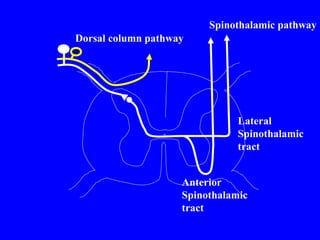
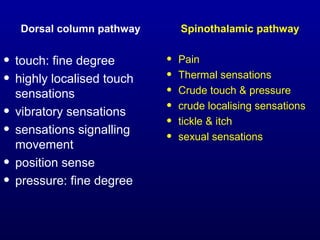
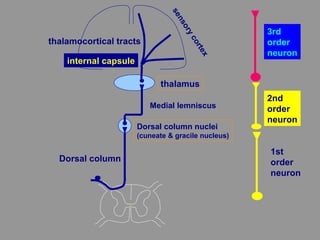
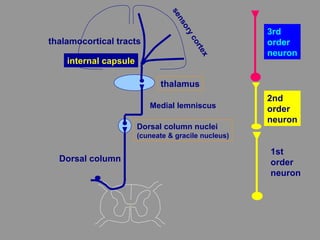
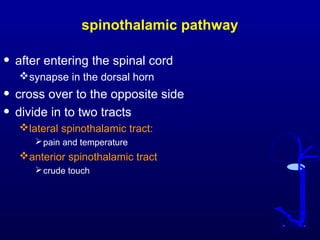

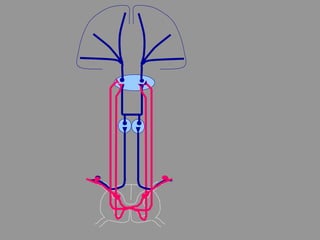
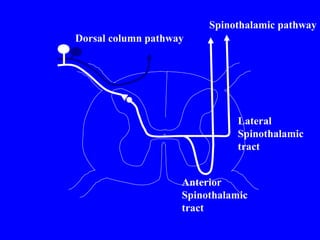
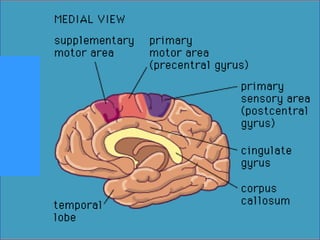
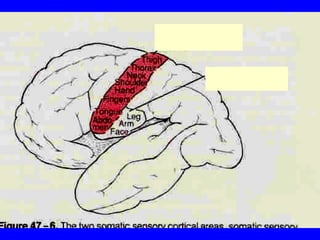
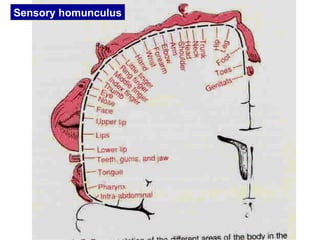

This document discusses the human sensory system, including sensory receptors, pathways, and cortex. It describes the different sensory modalities and sensations. The main sensory pathways are the dorsal column-medial lemniscus pathway and spinothalamic pathway, which transmit signals from receptors to the thalamus and sensory cortex. Within the cortex, different body regions are represented in a distorted map called a sensory homunculus. The document provides details on various mechanoreceptors, transduction of stimuli to action potentials, and coding of sensory information.























































































