Downloaded 260 times

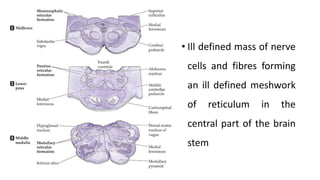
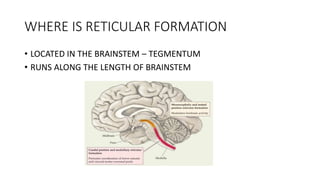
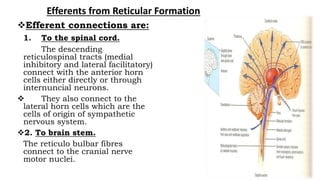
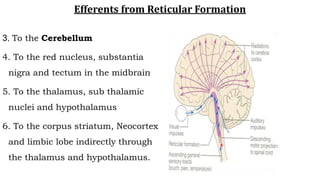
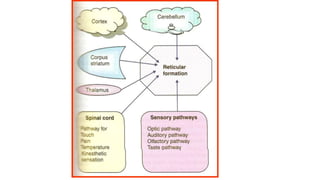
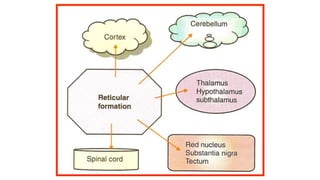
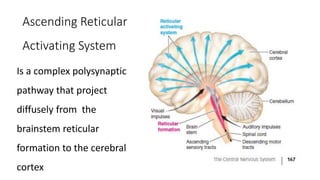
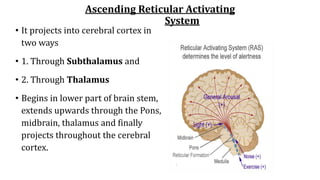
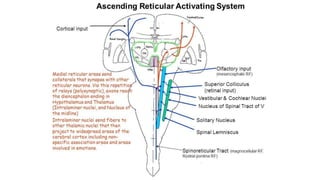
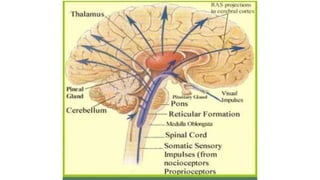


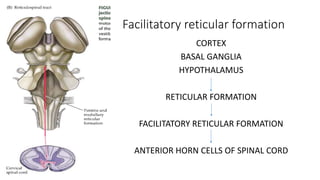



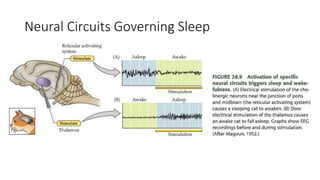

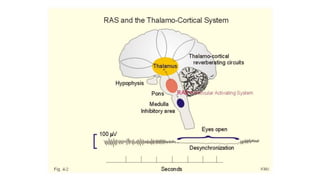

1). The reticular formation is an ill-defined region in the brainstem comprising neurons and fibers that extends from the spinal cord to the thalamus. It is involved in arousal, attention, sleep-wake cycles, and autonomic functions. 2). The ascending reticular activating system projects from the brainstem reticular formation to the thalamus and cortex, promoting wakefulness. The descending pathway projects to the spinal cord and is involved in motor function. 3). The reticular formation receives inputs from sensory systems and projects to the thalamus, hypothalamus, and spinal cord. It regulates functions like muscle tone, respiration, cardiovascular control, and endocrine secretion.














































































